
The Sugar and Rice Diet That Reversed “Irreversible” Disease
Kempner Was Right: Disease Is a Fuel Problem

In 1939, a German doctor at Duke University did something that should have killed his patients. He fed diabetics, kidney failure cases, and people dying of malignant hypertension a diet built around white rice, fruit juice, and table sugar. Some of them ate up to 500 grams of pure sugar a day. Their fasting blood sugar dropped. Their insulin doses fell or disappeared. Their failing kidneys started working again. Their malignant hypertension reversed. And in many of his diabetic patients, the damage to their retinas, the kind we still treat today by burning the retina with lasers because we assume it’s permanent, started to heal.
His name was Walter Kempner. He treated more than 17,000 patients with this diet over four decades. The results sit in old medical journals, mostly forgotten, because they break almost every nutritional rule we’ve been taught since.
For most of the last 80 years, the Rice Diet has been a historical curiosity. That changed recently. In 2019, a team at Duke and the Hasso Plattner Institute in Germany began digitizing Kempner’s handwritten patient charts. They built a database of 17,487 patients with more than 110 health markers each, plus 55,332 retinal photographs. Three peer-reviewed papers have come out of this project so far, in BMJ Nutrition Prevention & Health (2024), in Hypertension (2026), and a long-term follow-up preprint (2026). The findings broadly confirm what Kempner reported. The healing was real, and it was bigger than even Kempner’s critics admitted at the time.
I want to walk through what actually happened. What it tells us about how cells work. What Kempner got right. And the one big assumption he built into the diet that probably limited the long-term results.
A scientist who studied how cells breathe
To understand why Kempner thought rice and sugar could heal end-stage disease, you have to know where he came from intellectually. Before he left Germany and landed at Duke in 1934, he trained in Otto Warburg’s laboratory in Berlin. Warburg won the Nobel Prize for showing that cancer cells lose the ability to fully burn glucose for energy. Healthy cells take glucose, run it through their mitochondria, and produce a lot of ATP along with carbon dioxide and water. Sick cells skip the mitochondrial step and ferment glucose instead, producing very little energy and a lot of lactic acid. Warburg’s whole career was about how cellular energy production fails in disease.
Note: A clarification worth making here, because Warburg’s work gets misused constantly. The fermentation pattern is something cancer cells do, not something sugar makes cells do. The damage to cellular respiration comes from other inputs, primarily polyunsaturated fats, chronic stress, inflammation, and impaired thyroid function, not from glucose itself. Glucose is the fuel that lets damaged cells recover, and we’ll see this play out in Kempner’s diabetic patients shortly. The “sugar feeds cancer” idea is a logical leap that Warburg himself never made.
Kempner absorbed this framework completely. His earliest research at Duke was on kidney cells starved of oxygen. He found that when kidney cells couldn’t breathe properly, they couldn’t process amino acids from protein. From this he built his whole clinical theory. Years later, he summarized it for skeptical Duke medical students this way: the problem with renal failure is the resulting metabolic dysfunction. The kidneys excrete waste products, amino acids, keto-acid metabolites, hydrogen ions, and salt, and all these things come from what people eat. Theoretically, you should be able to make sick patients better by reducing the amount of work the kidneys have to do.
The reason this matters for diabetes and retinal damage too, not just kidney disease, is that all three conditions share the same underlying machinery. The kidneys, the retinas, and the heart are the organs in the body most dependent on dense networks of tiny capillaries. The kidney is essentially a giant capillary filter, with about a million microscopic vessel-balls (glomeruli) doing the work of cleaning blood. The retina has the highest metabolic rate per gram of any tissue in the body, fed by another dense capillary network. When something damages capillaries systemically (high blood pressure pounding them mechanically, chronic high blood sugar stiffening their walls through glycation, polyunsaturated fats generating oxidative damage in the vessel lining), all three organs fail in parallel. A diabetic with retinopathy almost always has some degree of kidney damage too. Malignant hypertension shows up at the same time in the retina, the kidneys, and the heart. These aren’t three separate diseases co-occurring. They’re three faces of the same accelerating crisis in the body’s smallest blood vessels.
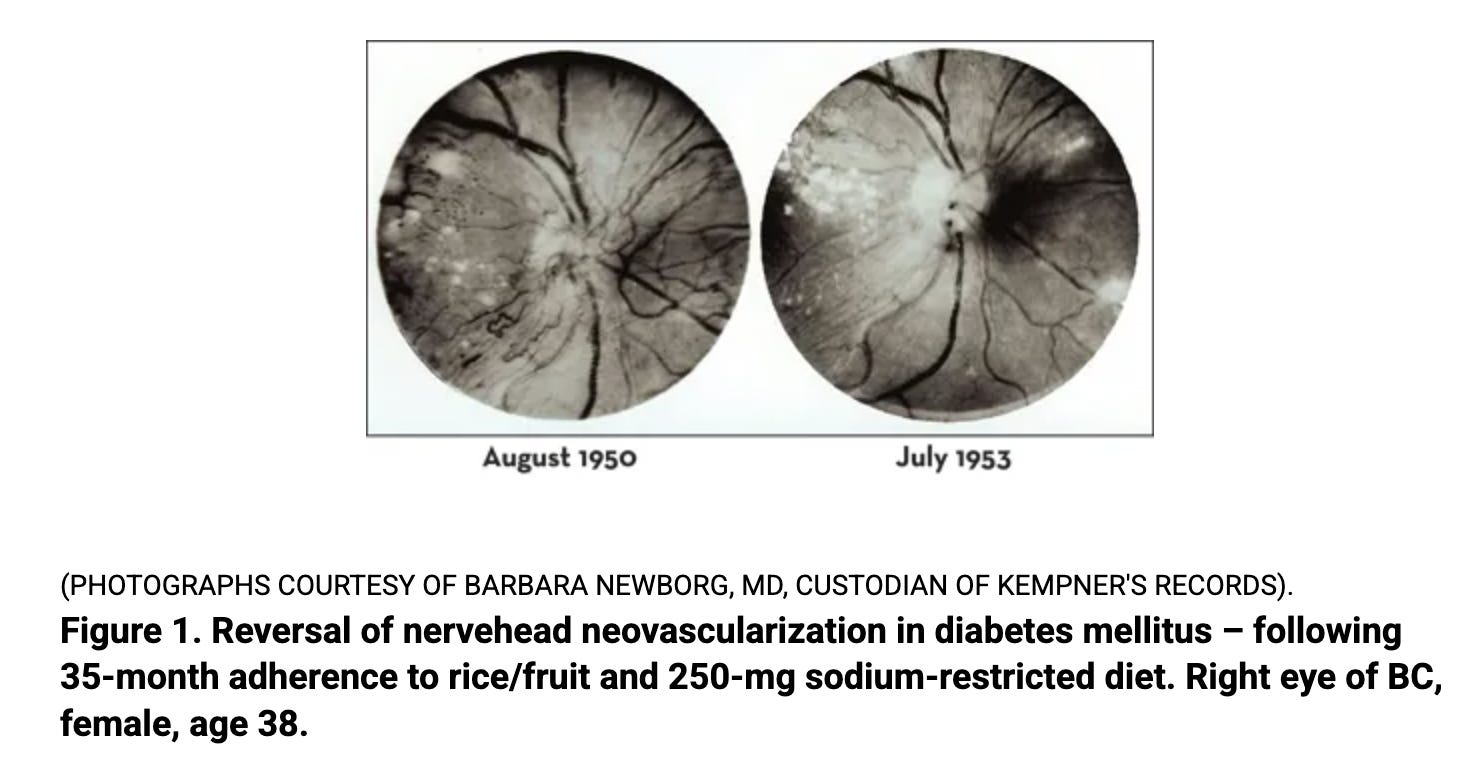
This is why Kempner’s “rest the kidney” theory worked for so much more than kidneys. Strip the diet down to the minimum metabolic load, and you don’t just relieve the kidney. You stop the systemic damage to capillaries everywhere. The retina, the kidney filter, and the heart muscle all get the same chance to repair, because they were all failing from the same cause. The retina was Kempner’s diagnostic window for this. He could photograph the back of the eye and watch the hemorrhages clear up week by week. The same healing was happening in the kidneys and throughout the cardiovascular system. The retina just let him see it directly.
So when he designed his therapeutic diet, he wasn’t picking foods based on tradition or taste. He was asking a specific question: what is the lowest possible metabolic burden you can put on a damaged cell while still keeping the body alive? His answer was rice, fruit, and sugar. These foods deliver glucose, the cleanest fuel a cell has, and almost nothing else. No nitrogen waste from breaking down protein. No fat fragments to interfere with glucose burning. Minimal sodium load. The cell could focus on healing instead of processing.
This is bioenergetic thinking decades before the term existed. Kempner was running clinical metabolic therapy without the modern vocabulary, drawing on the same scientific lineage that Ray Peat would later make popular.
What the diet actually looked like
Kempner published the original protocol in JAMA in 1944. It provided about 2,000 to 2,400 calories per day, roughly 95% of which came from carbohydrate. Protein was around 20 grams, mostly from the rice itself. Fat was almost nonexistent, around 2 to 3% of calories. Sodium was held under 150 mg per day, which is about a tenth of what most people eat. Fluid intake was capped at 700 to 1,000 ml. A multivitamin covered the B-vitamin gaps that come from eating polished white rice.
Sugar was given freely, with no upper limit. Most patients consumed around 100 grams a day, but some took in up to 500 grams to maintain their body weight. Underweight patients were fed more. The whole purpose was healing, not weight loss.
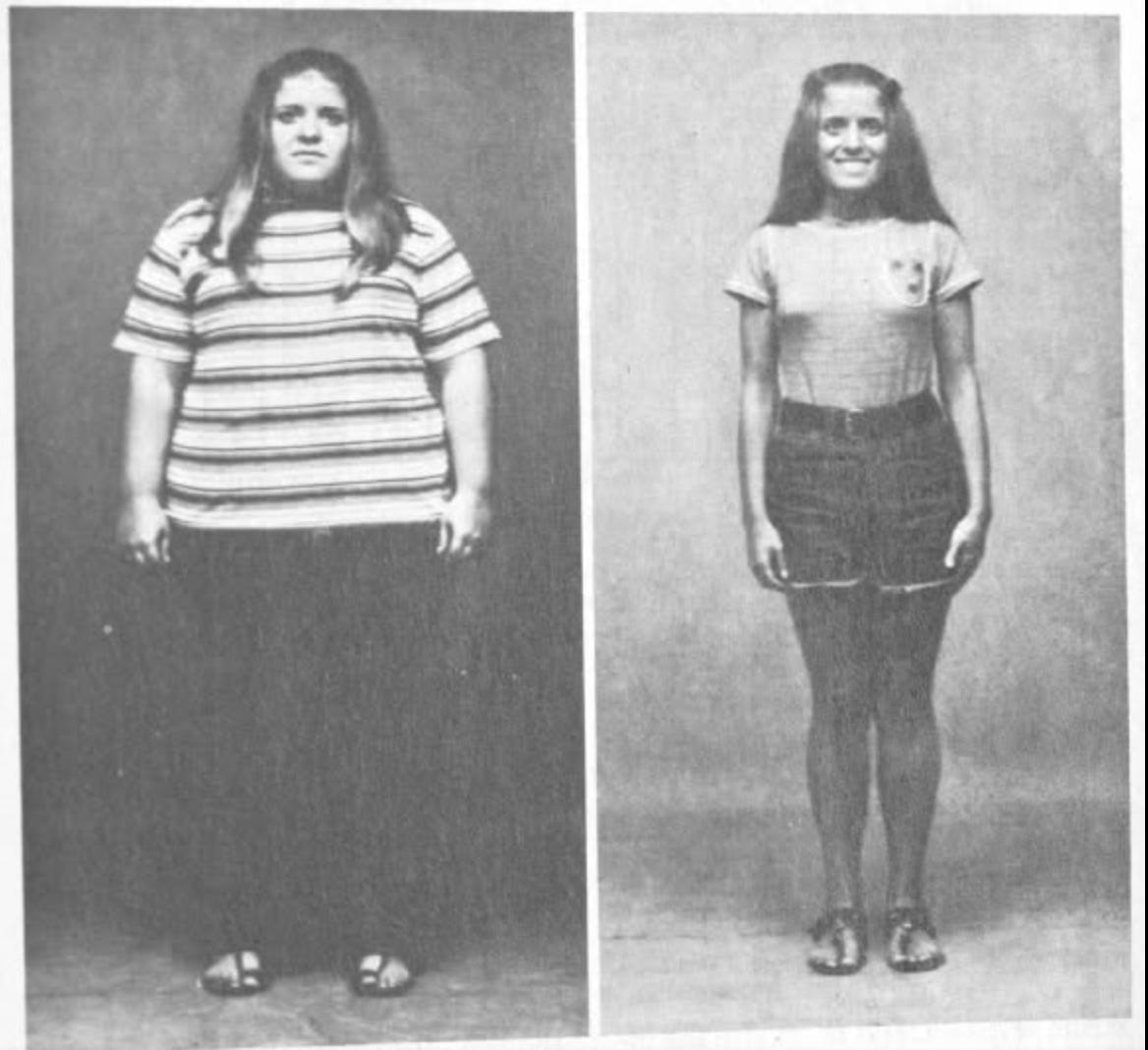
This distinction matters because there is a second version of the Rice Diet that came later. In the 1950s and 60s, when Kempner started using the diet for severe obesity, he ran it at 800 to 1,200 calories per day. That version produced the dramatic weight loss numbers people sometimes cite, average losses of 140 pounds and more. The interesting findings, the kidney recovery, the diabetes reversal, the malignant hypertension cures, all came from the original 2,400 calorie version where patients were not in a deficit. When you read about the Rice Diet, knowing which version is being discussed changes everything about what the data mean.
What the new database analysis shows
The 2024 BMJ paper analyzed 15,344 participants who stayed in the program for at least five days. The 2026 Hypertension paper zeroed in on 544 patients with malignant hypertension, the worst-prognosis group. Some of the headline numbers:
In severe hypertensives, median systolic blood pressure dropped from 205 mmHg to 143 mmHg over the program. Median follow-up was 162 days. Five-year survival in this group, where untreated median survival was historically 6 to 18 months (!), was 71.6%. In the malignant hypertension cohort specifically, systolic pressure fell by a median of 35 mmHg within the first 4 weeks of treatment.
These numbers are not subject to recall bias or self-reporting. The team used 24-hour urine chloride measurements as a hard biomarker of dietary adherence. Median urine chloride dropped 13-fold during the program, confirming patients were biologically on the diet, not just claiming to be.
The diabetes finding that should have changed medicine
Of all Kempner’s results, the diabetes outcomes are the most important.
In 1958 he published a study on 100 diabetic patients treated with the high-carbohydrate diet. Conventional medicine at the time, much like today, viewed diabetes as a disease of glucose handling. The standard treatment was to restrict carbohydrate, because eating sugar raises blood sugar, and high blood sugar is what kills diabetics. Feeding sugar to a diabetic was considered close to malpractice.
Kempner went ahead with it anyway because his theory said something different. He didn’t think diabetes was caused by sugar. He thought diabetes was caused by cells that had lost the ability to burn glucose properly. If you could restore cellular energy production, the body would handle sugar normally again. The way to restore cellular energy production was to clear out everything that interfered with it, especially dietary fat, and supply the cell with its preferred fuel.
The results vindicated him. Fasting blood glucose came down. Insulin requirements dropped, and in many cases patients came off insulin entirely. Of the 100 diabetics, almost half had retinopathy at the start of the study, and most of those had the most severe form, retinitis proliferans. After an average of 22 months on the diet, roughly 30% showed bilateral improvement on fundus photography, another 16% improved in one eye. Roughly half saw their diabetic eye damage halt or reverse.
Retinopathy is the eye disease where chronic high blood sugar damages the tiny blood vessels in the retina, eventually causing blindness. Modern ophthalmology treats it with laser surgery that deliberately destroys parts of the retina to stop the bleeding. We do this because we believe the damage cannot be undone. Kempner reversed it in roughly a third of his retinopathy patients with rice and sugar.
The mechanism makes sense if you think about diabetes the way Kempner did, as a fuel-handling failure rather than a sugar problem. Excess fatty acids in the blood, especially polyunsaturated ones, suppress glucose oxidation through what’s called the Randle cycle. The cell, flooded with fat fragments, stops burning glucose and starts ignoring insulin’s signal. Blood sugar rises not because too much sugar came in, but because the cell can’t use what’s there. Stress hormones from chronic inflammation make this worse. Cortisol stays elevated, telling the liver to keep producing glucose around the clock through gluconeogenesis, even when blood sugar is already high. Cortisol also tells fat tissue to release fatty acids into the blood, which then compete with glucose at the cellular level and worsen the Randle cycle problem. Blood sugar rises further, the cell still can’t burn it, and the inflammatory signal stays elevated because high blood sugar is itself inflammatory. The loop closes on itself and runs indefinitely.
When you remove almost all the fat from the diet, the Randle cycle reverses. The cell starts burning glucose again. Insulin sensitivity returns. Blood sugar normalizes because the cell is finally pulling glucose in and using it. The capillaries in the retina, no longer damaged by chronically elevated blood sugar and the inflammation that comes with it, begin to heal.
The opposite approach to Kempner’s, the one that’s popular today, is to remove carbohydrate entirely. Strict keto diets treat diabetes by cutting out the sugar so blood sugar can’t rise. On the surface this makes sense. If sugar is the problem, remove it. But this misunderstands what’s actually happening in a diabetic body, and it creates a different problem most keto advocates don’t talk about.
Your blood sugar has to stay in a narrow range. Your brain, your red blood cells, and parts of your immune system require glucose to function. They cannot run on ketones. So when you stop eating carbohydrate, your body has to make its own glucose from scratch, using a process called gluconeogenesis. The liver pulls amino acids out of your muscle, breaks them down, and assembles them into glucose. This runs around the clock on keto because your blood sugar can never be allowed to crash.
The catch is that gluconeogenesis requires elevated cortisol and adrenaline to drive it. These are stress hormones. So a keto diet keeps your stress hormone system chronically activated, because that’s the only way to keep generating glucose internally. This is why people on long-term keto often develop poor sleep, anxiety, hair loss, cold hands and feet, suppressed thyroid function, muscle wasting, and (in women) loss of menstrual cycles. The body is in a constant low-grade emergency state, fueling itself by breaking down its own tissue under the command of stress hormones.
People often feel sharp and energetic on keto initially. There are two reasons for this. First, most people coming to keto were eating a lot of seed oils, processed food, and erratic meals, so any structured diet feels like an improvement. Second, elevated cortisol and adrenaline produce a feeling of focus and energy in the short term. The cost shows up months or years later, by which point most people have built an identity around the diet and find it hard to recognize the connection.
Kempner’s results show the opposite logic works better. Don’t remove the glucose. Remove the obstacles that’s blocking your cells from using glucose properly. Supply abundant clean carbohydrate so your stress hormone system can stand down. The body stops needing to manufacture its own emergency fuel, the cells start burning glucose normally again, and insulin sensitivity returns from the inside. This is why the Rice Diet reversed diabetic complications that no keto study has ever matched.
This is the finding that should have rewritten diabetes treatment. Instead it sat largely ignored for half a century, partly because by the time Kempner published, the field had committed to a different theory, and partly because telling diabetics to eat sugar sounded too crazy to take seriously.
If you ever try this diet
None of this means the Rice Diet is an ideal way to eat. It is a powerful short-term intervention for end-stage disease. It works because removing chaos in a deeply sick body produces fast results. But several features of the diet would have caused real problems if you tried to live on it long-term, and one of them rests on an assumption I want to push back on directly.
Start with the obvious nutritional gaps. The diet contained almost no fat. Some saturated fat from sources like butter, coconut oil, or beef tallow supports thyroid function, hormone production, and cell membrane integrity. Running on near-zero fat for months would slowly suppress steroid hormone production, which matters for energy, repair, and resilience. The diet was also extremely low in calcium, providing around 140 mg per day when adults need closer to 1,000 mg. Long-term, that drives parathyroid hormone elevation, bone loss, and soft tissue calcification. Calcium, mostly from dairy, is one of the most metabolically important minerals there is, and the Rice Diet missed it entirely.
The protein content was 20 grams a day, which offloads the kidneys but produces muscle wasting and immune compromise over time. Most adults need 80 to 100 grams from sources like dairy, gelatin, shellfish, and muscle meat to maintain lean tissue and produce the enzymes the body runs on. The diet also relied on a multivitamin to prevent from B-vitamin deficiency, which is a tacit admission that polished white rice and sugar can’t sustain a person nutritionally without supplementation. The healing effect was real, but it came from removing burdens, not from the foods themselves being optimal.
The salt question
The most controversial part of Kempner’s protocol was the extreme sodium restriction, under 150 mg per day. He treated salt the same way he treated protein and fat: as another excretory burden the kidney had to handle, so minimizing it fit his “rest the kidney” framework. The new Duke papers in 2024-2026 read this as evidence that extreme sodium reduction is safe and effective. I want to walk through why this conclusion does more work than the data actually supports.
First, the methodological problem. Kempner stripped sodium, protein, and fat all at once, added bed rest, daily medical supervision, weight loss in many patients, and removal from chaotic home environments. Then he reported the BP improvements. There is no way to separate out which intervention did which fraction of the work. The new Duke analyses, despite using rigorous biomarkers for adherence, run into the same wall. They cannot tell you that low salt was the active ingredient because every patient also had low PUFA, low protein, abundant clean carbohydrate, and constant clinical attention.
Second, what we know from physiology. When sodium intake drops well below physiological needs, the body fights back. Aldosterone rises. Renin rises. Adrenaline rises. These are stress hormones that retain sodium and raise blood pressure. The body doesn’t quietly accept low sodium as a healthy state. It treats sodium deprivation as a threat and mobilizes the same hormonal cascade that drives long-term cardiovascular damage. Several large studies have found that very low sodium intakes are associated with worse cardiovascular outcomes and higher all-cause mortality, not better. The acute BP drop from sodium restriction comes at the cost of chronic stress hormone elevation, and the long-term ledger is at best a wash and probably negative.
Third, when you push sodium too low, oxidative metabolism suffers, the very thing Kempner was trying to optimize. None of this is measured in the Rice Diet papers. They tracked blood pressure, weight, and urine chloride. They did not measure thyroid function, metabolic rate, or stress hormone levels. So the broader metabolic costs that bioenergetic thinking would predict are not refuted by the data. They are simply outside what the studies looked at.
Fourth, who actually benefits from sodium restriction. Some people do. Patients with significant fluid retention, advanced kidney disease, or volume-overloaded malignant hypertension can have an acute volume problem where lowering sodium meaningfully reduces vessel pressure. Kempner’s malignant hypertension cohort likely included a lot of these patients. That’s part of why the diet worked acutely. But this is a narrow clinical population, not the general public. Extrapolating from “low sodium helped patients with end-stage volume-overloaded hypertension” to “low sodium is good for healthy people” is exactly the kind of leap the data don’t support.
For most healthy people, salting food to taste with adequate sodium (around 3 to 5 grams per day) supports metabolism, keeps stress hormones in check, and does not cause hypertension. Salt restriction is not a free intervention. It comes with metabolic costs that the standard public health messaging consistently ignores. The Rice Diet’s sodium restriction was an artifact of Kempner’s theory, not a tested variable, and reading the diet’s success as proof that low salt is good for you misreads what the data can and cannot show.
The honest summary is this. Most of the Rice Diet’s healing came from low PUFA, reduced protein burden, abundant clean glucose, and removal of dietary inflammation. These are the metabolic levers worth pulling. The salt restriction was Kempner’s hypothesis, not a separately validated component, and a version of the same diet with normal physiologic salt intake would likely produce similar healing without the stress-hormone consequences and acute electrolyte problems Kempner had to manage.
Note: There’s a related point worth making here. Kempner also restricted fluid intake to 700-1000 ml per day, which sounds extreme until you understand why. He had to. When sodium intake drops well below physiological need but water intake stays normal, blood sodium gets diluted, leading to hyponatremia so the fluid restriction was a workaround for a problem the salt restriction created.
This actually flips the modern “drink 8 glasses of water a day” advice on its head. Your thirst signal tracks both water needs and sodium status. When you salt food to taste and drink to thirst, the body manages fluid balance with very high precision. When you force extra water while keeping salt low, you dilute your electrolytes and stress the kidneys, which is why so many people who diligently follow hydration advice end up with low energy, cold hands, frequent urination, and worse sleep instead of the vitality they were promised.
Translating this into actual life
You don’t need to live on rice and sugar to apply what Kempner discovered. The principles that powered his results translate into something much more livable, and much more nutritionally complete.
Keep polyunsaturated fat low. This is the single most important change for most people. Industrial seed oils, excess nuts, and large amounts of fatty fish accumulate in tissues over years and impair cellular glucose handling long after you stop eating them. Reducing them is more important than any supplement.
Eat adequate clean carbohydrate. Ripe fruit, fruit juice, honey, dates, white sugar in homemade sweets or coffee, milk, well-cooked starches. Carbohydrate is the fuel your mitochondria prefer, and it lowers stress hormones the way nothing else does.
Keep protein moderate, around 80 to 100 grams a day, from sources that support metabolism without stressing the gut or liver. Dairy, gelatin, shellfish, eggs, muscle meat.
Salt to taste with real salt. Your body knows how much it needs.
Get enough calcium, mostly from dairy. Sleep, sunlight, warmth, gentle movement.
That’s a metabolically supportive way of eating that captures the engine behind Kempner’s results without the nutritional gaps that made the original diet unsustainable. The same principles, made livable.
Loved this piece! I'm going to ask this here because I keep searching for an answer: I see a lot of folks promoting white sugar (on its own or, like you said, in home made baked goods, with coffee, etc...) as a clean energy source for the body. On the other hand, I am inundated everywhere I turn with warnings about how inflammatory refined sugar is. I have RA, and am constantly told I need to cut out ALL refined sugar because it is so inflammatory. I'm having a lot of trouble squaring these two realities and feel like I'm missing some (maybe obvious??) piece of the puzzle. Thank you for any insight you could provide.
I think I am giving up--I have completely shifted my diet to whole grains, fresh veggies & fruits, mostly chicken, salmon, tofu, eggs & beans for protein. No white flour, no sugar, no potatoes, no white rice. Im tired.