
You Are Getting Shorter
The real reasons behind height loss and chronic back pain, why both start long before old age, and what you can actually do about them.

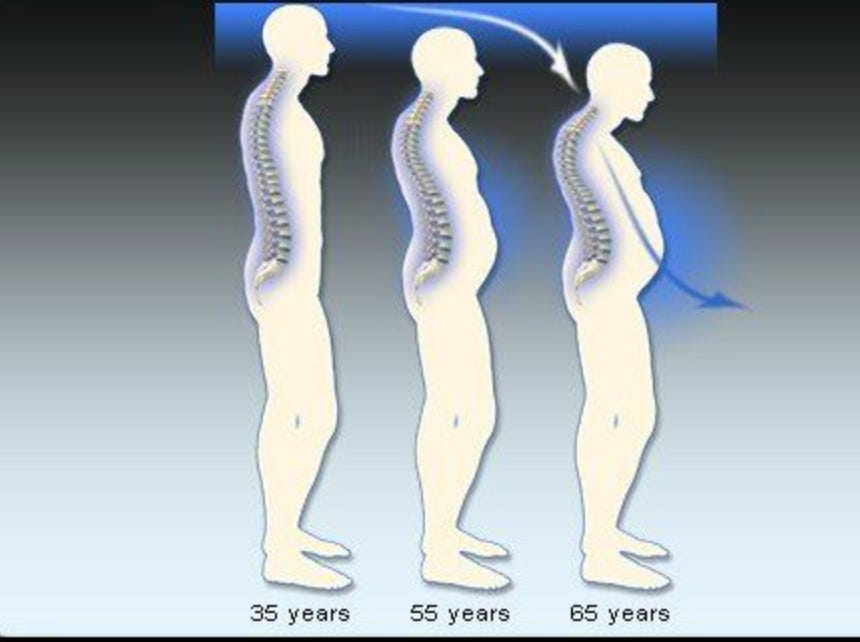
Recently I was going through some old family photos. Landed on one from a recent gathering and stopped. My brother, who spent his 20s jokingly complaining that our father was taller than him, was now standing at exactly the same height as our dad.
Our father is in his late sixties. My brother is in his early forties. Nothing dramatic had happened. No illness, no injury. My father had just quietly, gradually, gotten shorter. And none of us had really noticed until that photograph.
That picture stuck with me because height loss is one of those things we accept as a given of aging. It is supposed to happen to old people. It is supposed to be gradual and mild. It is supposed to be out of your hands.
Those assumptions fall apart once you look at what is actually happening inside the body. The structural changes that cause people to shrink are not random and they are largely not inevitable. A significant portion of what most people lose is preventable, and some of it starts in your thirties, long before anyone warns you it is coming.
The same structural deterioration that causes height loss is also the source of the chronic back pain, morning stiffness, and postural fatigue that most people are told to just manage. Same mechanisms, same metabolic roots, same protocol to address them. That is what this article covers.
How Much Taller Are You in the Morning?
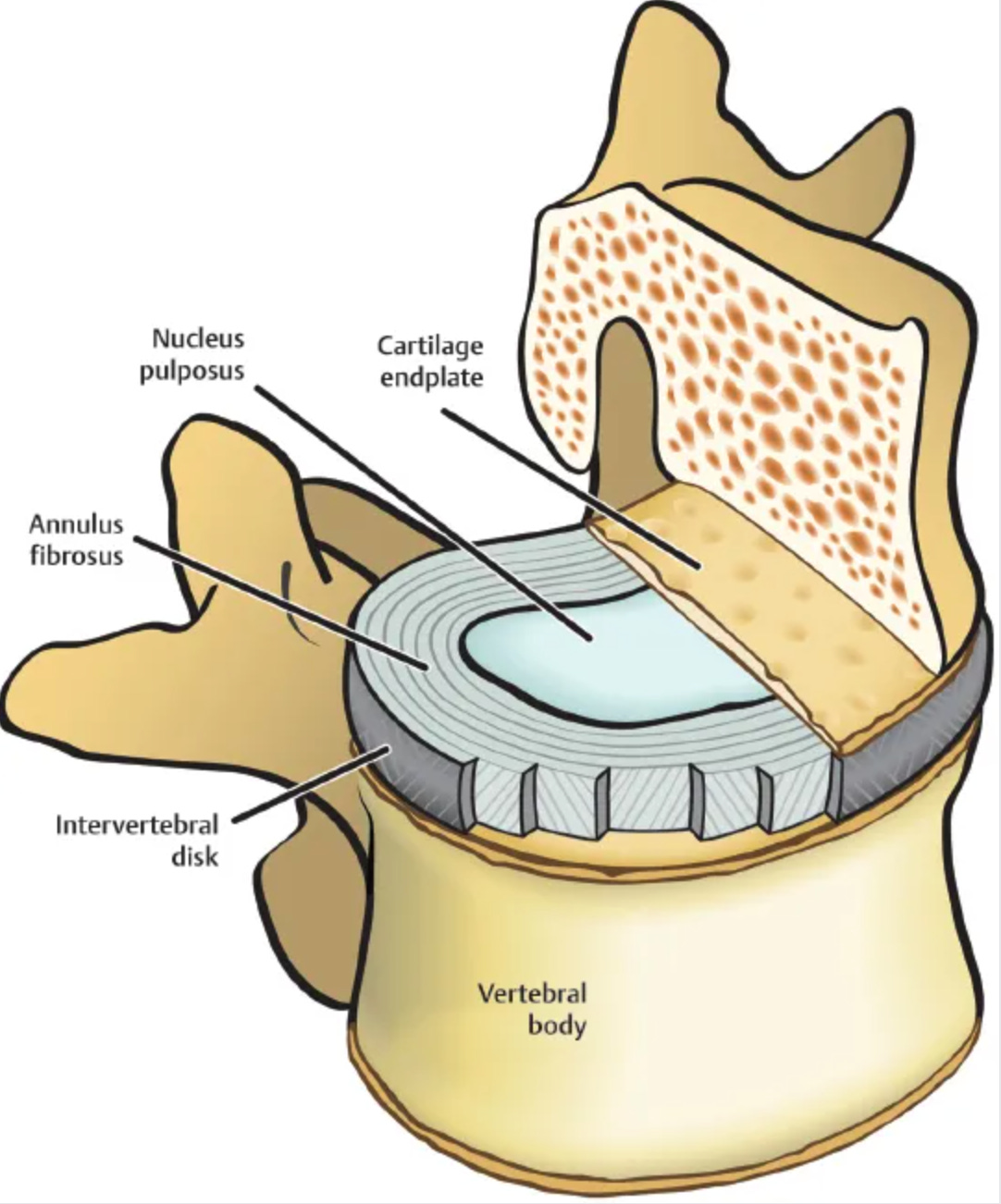
You are measurably taller when you wake up than when you go to bed. The difference is consistently measured at roughly 1 to 2 centimeters. You see, while you sleep horizontally, your intervertebral discs rehydrate. These discs sit between each of your vertebrae like small hydraulic cushions. During the day they lose fluid under the compressive load of being upright. Without gravity constantly squeezing them overnight, they absorb water and expand back toward their full height. By morning, the spine is longer.
As the day progresses and you resume loading the spine with sitting, standing, and moving, fluid is pushed back out and you return to your daytime height. This is normal. It happens every day throughout your life.
The problem starts when it stops being fully reversible. When the discs are chronically dehydrated, when the cartilage matrix has degraded, when the fluid-holding structures are damaged, morning rehydration becomes incomplete. The overnight gain gets smaller. That is when disc degeneration has already started, and it is also when morning stiffness stops being a five-minute inconvenience and starts taking half an hour to clear.
What You Are Actually Made Of, Height-Wise
Height is not just the length of your leg bones (obviously). A substantial portion comes from the 23 intervertebral discs in your spine. Each disc is roughly 7 to 10 millimeters thick when healthy. The center of each disc, called the nucleus pulposus, is essentially a gel that is 70 to 90% water when you are young. This pressurized core gives the disc its spring, its shock-absorbing capacity, and its height contribution.
Add up all 23 discs and they contribute roughly 10–15 cm to the length of the spine. Disc degeneration alone accounts for roughly 1 to 3 centimeters of loss over a lifetime. When you add vertebral compression and postural muscle decline, total height loss by the seventies typically runs 3 to 5 centimeters in men and 5 to 8 centimeters in women, with some losing considerably more. The visible shrinking, the forward lean, the slightly compressed look, comes primarily from here.
The rest of the height story involves the vertebral bones themselves, which can slowly compress if their internal structure weakens, and the muscles that hold the spine upright. A spine supported by strong paraspinal muscles sits taller than one that slumps because the supporting musculature has given way.
Height loss happens through three separate but interconnected mechanisms, each with its own metabolic drivers.
Why Women Lose More
On average, women lose more height over their lifetime than men do. Understanding why means looking at what is actually different between female and male bone and disc biology, not just pointing at menopause as if that explains everything.
The Estrogen and Progesterone Picture
Estrogen is the best-known protective hormone for bone. It suppresses osteoclasts, the cells that break down bone tissue. When estrogen falls at menopause, osteoclast activity accelerates and bone loss speeds up. Bisphosphonate drugs were designed to pharmacologically mimic this effect, slowing osteoclasts down. But estrogen does not work alone in bone metabolism, and bisphosphonates do not replace the other side of the equation.
The other side is progesterone. Progesterone actively stimulates osteoblasts, the cells that build new bone. Bone remodeling requires both sides working in balance. Research by endocrinologist Jerilynn Prior at the University of British Columbia documented that progesterone deficiency begins producing measurable bone loss in premenopausal women, years before estrogen declines. This finding was largely sidelined in favor of the cleaner estrogen narrative. Current guidance focuses almost entirely on estrogen and the menopausal transition, while years of progesterone insufficiency that preceded it go unaddressed.
Cycles that are technically present but anovulatory, meaning ovulation is not occurring, produce no progesterone in the luteal phase. This is common in women under chronic stress, at low or excessive body weight, or with thyroid disruption. The bone loss starts quietly, long before any conversation about menopause. By the time a woman reaches her fifties and her doctor first mentions bone density, she may have already lost significant trabecular bone from a decade or more of progesterone insufficiency.
For men, the hormonal picture is different but the principle holds. Testosterone and its local conversion to estradiol within bone tissue both contribute to bone density. Low testosterone reduces anabolic signaling across muscle and bone simultaneously. The muscle loss and bone loss that accelerate together in men through their fifties and sixties are not coincidentally linked. They run through the same hormonal decline in the same tissue.
Smaller Starting Reserves
Women also begin adulthood with lower peak bone mass than men. Peak bone mass is reached around age 25 to 30. Men’s higher testosterone levels during puberty and early adulthood drive more bone development during that window, so they enter middle age with a larger structural reserve to deplete. The same rate of age-related loss hits women harder in absolute terms simply because they had less to lose.
Disc biology follows the same pattern. Estrogen has a protective effect on disc cells, so postmenopausal women show accelerated disc desiccation compared to age-matched men. This directly compounds the spinal height loss picture.