
The Old Clinical Trick for a Sluggish Gallbladder
An old sanatorium procedure for stimulating gallbladder contraction, draining stagnant bile, and restoring flow


A single procedure, done at home in two hours, can empty a gallbladder that has been sluggish for years. No surgery, no prescription. In Eastern European sanatoriums this has been standard care. In American medicine it does not exist.
It is called tubazh (or tubage).
If you read my last piece on bile, you already know why this matters. Bile helps clear hormones, carries fat-soluble waste out through the intestine, and allows you to absorb the fat-soluble nutrients needed to build steroid hormones. When bile slows, all of that slows with it. The downstream pattern can show up as estrogen dominance, jaw acne, sluggish thyroid, cold hands, fat intolerance, brain fog, stubborn weight, hormonal acne, low vitamin D that will not come up, melasma, dull skin, headaches, and histamine reactions. The list goes on.

The article on bile laid out a protocol to restore flow through food, supplements, and lifestyle. It works, and it builds the foundation that everything else sits on top of. Tubazh is what accelerates it. Done correctly, on a system that has been prepared, it can move bile flow faster than food and supplements alone.
What tubazh actually is
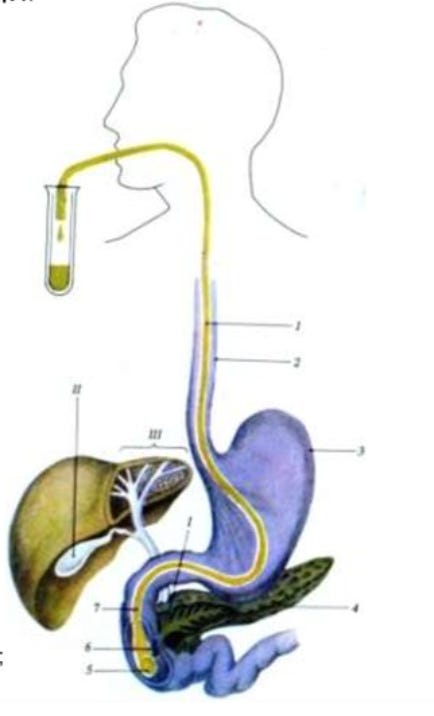
The original procedure uses a thin tube passed through the mouth into the small intestine to drain bile directly. That version still exists in clinical settings and is called probe tubazh or duodenal sounding.
The version this article is about, and the version most people use today, is called blind tubazh, probeless tubazh, or in the original Russian medical literature, tubazh by Demyanov. There is no tube. The bile drainage happens through the body’s own machinery, triggered by an oral choleretic and supported by heat applied to the liver area.
I did this procedure many times in both versions. The one with the tube is no fun, honestly, though it remains genuinely useful for people with biliary dyskinesia. You swallow a thin rubber tube, the doctor or nurse waits until it reaches the duodenum, and the bile drains directly through it. This was a standard pediatric procedure where I grew up. The swallowing was the worst part. Blind tubazh was developed precisely to keep the medicine and drop the misery.
Please note this is not the same as the dramatic olive oil and lemon juice flushes that have circulated through alternative medicine for decades. Those protocols are aggressive, often produce what look like stones but are actually saponified soap masses, and have a documented record of causing real complications. Tubazh works through the body’s natural cholecystokinin signaling and gallbladder contraction reflex, not through a forced extraction. The medical tradition that developed it has used and refined it for almost a century.
Where it came from
In 1909, the German-born American physician Ehrenfried Max Einhorn developed one of the first thin flexible tubes that could be passed beyond the stomach into the small intestine to collect bile for analysis. A year later, in 1910, Morris Gross developed his own variant. These were diagnostic tools, used to study bile composition, look for parasites, and assess gallbladder function.
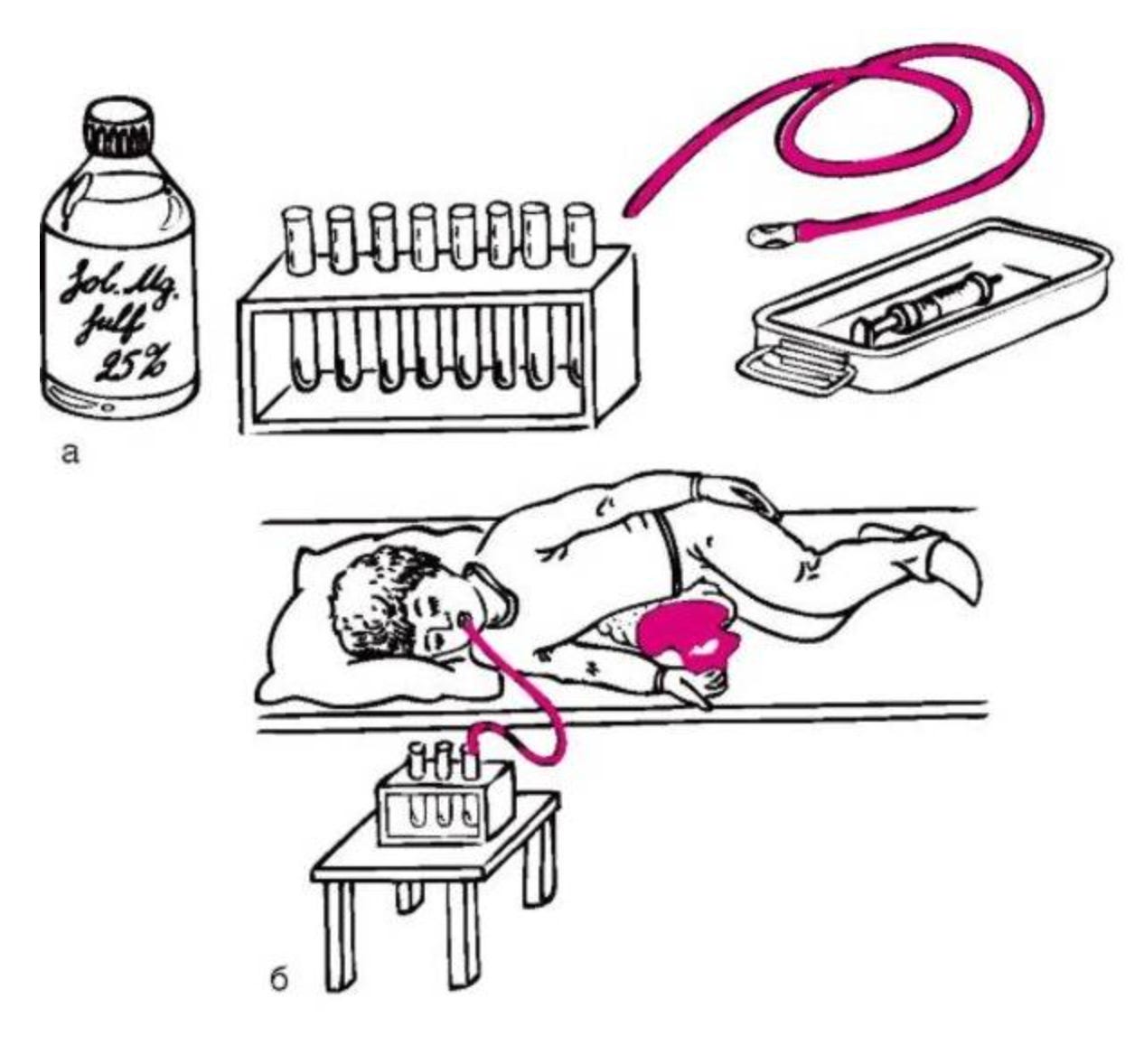
In 1923, the American physician B. B. Vincent Lyon published a monograph called Non-Surgical Drainage of the Gall Tract. Lyon noticed that when magnesium sulfate was introduced through the duodenal tube, it stimulated bile drainage, and at the same time cleared out stagnant bile, mucus, and inflammatory products. He proposed that regular therapeutic drainage, beyond diagnostic sampling, could treat chronic biliary inflammation and stagnation. This was the beginning of therapeutic tubazh.
In the 1920s and 1930s, duodenal sounding spread across European medical practice. It was used in German, French, and Soviet clinics. But the procedure had a problem: it required swallowing a tube, which most patients found extremely unpleasant (can confirm), and it required clinical infrastructure to perform safely.
Then in 1948, the Soviet physician G. S. Demyanov published a method that changed everything. Demyanov demonstrated that the same therapeutic effect could be achieved without any tube at all. By giving an oral choleretic agent (originally magnesium sulfate dissolved in warm water) and applying heat to the right upper abdomen while the patient lay on the right side, the gallbladder would contract reflexively and empty its contents into the duodenum. This was tubazh by Demyanov, also called blind tubazh, because it spared patients the discomfort of the tube.
From there it spread through the postwar sanatorium systems of Russia, Ukraine, Belarus, Czechoslovakia, Poland, Hungary, Romania, Bulgaria, and East Germany. The famous mineral water resorts (Essentuki and Pyatigorsk in Russia, Truskavets and Morshyn in Ukraine, Karlovy Vary in the Czech Republic) built whole protocols around tubazh combined with their local mineral waters. The procedure became standard care for biliary dyskinesia, chronic non-calculous cholecystitis, and a range of liver conditions across multiple medical traditions.
Today, tubazh remains part of sanatorium and gastroenterology practice in parts of the same medical tradition. It is taught in pediatric gastroenterology textbooks. The 2013 textbook by Kildiyarova and Lobanov, used in medical schools, recommends tubazh by Demyanov 2-3 times per week, as a course of 10-12 procedures, combined with oral choleretics for two weeks per month over six months.
In the United States and most of Western Europe, tubazh never crossed over. The reason has more to do with how American medicine evolved away from balneotherapy and toward pharmaceutical and surgical management of biliary issues than with anything wrong with the procedure itself. By the 1960s and 70s, American medicine had largely abandoned bile-flow-focused treatment in favor of either watchful waiting or surgical removal. The mechanistic research that supports tubazh continued in American journals, but the therapeutic application stayed in the medical traditions that had developed it.
How it works
Tubazh works because three physiological mechanisms get triggered simultaneously: the gallbladder contracts, the sphincter of Oddi relaxes, and gravity assists the drainage. Each of these has been documented in mainstream Western medical literature, even though the combined therapeutic application stayed elsewhere.
CCK release contracts the gallbladder
When magnesium sulfate, sorbitol, xylitol, or certain bitter mineral waters reach the duodenum, they trigger the release of cholecystokinin (CCK), the hormone that signals the gallbladder to contract. This is the same hormone released when you eat a fatty meal, but in tubazh the release is more concentrated and sustained because the choleretic is given on an empty stomach with no food to dilute the signal.
Wiener and colleagues, publishing in the Annals of Surgery in 1981, demonstrated direct correlation between blood CCK levels and gallbladder contraction in humans after oral magnesium sulfate. The 1983 follow-up study confirmed the same. Magnesium sulfate is a documented cholecystokinetic agent in mainstream Western literature.
Magnesium relaxes the sphincter of Oddi
The sphincter of Oddi is the muscular gate at the end of the common bile duct that controls how bile leaves the duct and enters the duodenum. If the sphincter is too tight, bile cannot flow out efficiently even when the gallbladder is contracting. This is one of the underrecognized causes of sluggish bile in hypothyroid patients, since T4 normally helps relax this sphincter.
Bergh and Layne, publishing in the American Journal of Digestive Diseases, reported that magnesium sulfate could relax the sphincter of Oddi when given orally or directly into the duodenum. More recent endoscopic research has confirmed that intraduodenal magnesium sulfate spray can reduce sphincter pressure and assist cannulation during ERCP when spasm makes access difficult.
So the same magnesium sulfate that triggers CCK release and gallbladder contraction also opens the gate at the other end of the duct. Both ends of the system get coordinated to drain together.
Heat increases local blood flow and supports smooth muscle relaxation
The hot water bottle on the right upper quadrant is not symbolic. Local heat application increases blood flow to the liver and gallbladder area, supports smooth muscle relaxation throughout the biliary tree, and provides comfort that helps the patient stay still in the right position for the full 90 to 120 minutes the procedure requires.
The main components of tubazh have mechanistic backing in mainstream Western research: CCK release, gallbladder contraction, and sphincter of Oddi relaxation. The clinical procedure combines these mechanisms into one coordinated event.
Who tubazh is for
Tubazh is one of the most useful procedures available for restoring bile flow when it has slowed down. It is mild, it is well-tolerated when done correctly, and the results are often dramatic. The clinical literature has used it for decades for the following situations.
• Chronic liver conditions where bile flow is sluggish but not obstructed.
• Chronic non-calculous cholecystitis (gallbladder inflammation without stones).
• Hypomotor (hypokinetic) gallbladder dyskinesia, where the gallbladder is sluggish and contracts weakly.
• Dysfunction of the sphincter of Oddi.
• Chronic constipation. A full intestine worsens bile stagnation and slows the whole enterohepatic loop.
• Postpartum women after breastfeeding has ended, where pregnancy hormones plus mechanical compression from the growing uterus often leave the biliary system sluggish for months after delivery.
• Obesity, which is consistently associated with impaired bile flow and altered bile acid composition.
• Periods of overeating or dietary excess, where the system needs help catching up.
• People without a gallbladder. Tubazh can still be done after cholecystectomy because bile flow through the ducts and sphincter regulation still matters. The mechanism shifts but the procedure is still useful.
If you saw yourself in any of these descriptions, or if you finished the bile article and recognized the symptom pattern in yourself, tubazh is likely an appropriate addition to your foundation work.
There are situations where tubazh should not be done. Tubazh stimulates gallbladder contraction and bile flow, so known gallstones require caution and should be handled clinically. Some experienced doctors report using tubazh even in patients with stones without seeing stone migration in practice, but this depends on the stone pattern, duct anatomy, symptoms, and the clinician’s judgment. This article is written for home use, so I am treating known gallstones as outside the scope of self-directed tubazh. Other contraindications include acute cholecystitis, acute pancreatitis, acute hepatitis, active peptic ulcer, severe liver disease, pregnancy and lactation, active menstruation, and recent abdominal surgery.
One pattern to know about. Most people have a sluggish gallbladder: dull heaviness in the right upper area, worse after fatty meals, slow digestion, fat intolerance that builds up over hours. This is what tubazh is for. There is another pattern where the gallbladder contracts too tightly against a stuck sphincter of Oddi, producing sharp cramping pain that comes and goes quickly, often triggered by stress. Tubazh is the wrong tool for that pattern. It may be uncomfortable and may not help. If your symptoms are sharp and cramping rather than dull and heavy, the right approach is relaxation and antispasmodics, not stimulation.
What tubazh actually produces
A successful tubazh produces several measurable and felt effects.
Mechanically, it empties the gallbladder. Stagnant bile that has been sitting and concentrating gets pushed out into the duodenum. The bile ducts get a wash of fresh bile flow, which may help move mucus, biliary sediment, and accumulated metabolites. The gallbladder refills with new bile from the liver, and the cycle of bile flow gets restarted from a cleaner baseline.
Symptomatically, many people report several things over the first 24 hours after tubazh. The right upper quadrant heaviness lifts, digestion may improve noticeably, and energy increases. In people whose skin symptoms are tied to impaired bile flow and estrogen recirculation, skin begins shifting over several weeks. Bowel function regulates. Morning stools often become darker and more formed.
Over a course of about 10 tubazh procedures spaced 5 to 7 days apart, the cumulative effect is significant. Sludge that was present at the start often improves measurably on follow-up ultrasound. Liver enzymes that were elevated typically come down. Many people report that hormonal symptoms tied to estrogen recirculation soften and that their relationship with food changes, with fewer crashes after fatty meals.
This is the same outcome the bile protocol produces over weeks. Tubazh accelerates the process by mechanically resetting bile flow, while the protocol provides the foundation that makes the reset hold.
What follows in the protocol
Below is the full procedure I use, drawn from sanatorium tradition with modifications based on what I have learned about supporting the system before, during, and after. The protocol covers the pre-tubazh requirements, the complete step-by-step procedure with timing, the choleretic options ranked by tradition and tolerance (including the actual sanatorium doses), the classical sanatorium course structure, troubleshooting, modifications for individual situations including post-cholecystectomy patients, and how tubazh fits with the bile protocol from the previous article.