
The Fluid That Decides How You Age, Detox, and Make Hormones
Countless metabolic problems trace back to it


The more I dig into metabolism, the more roads lead to the same place.
Every time I trace a problem backwards, whether it is hypothyroidism, estrogen dominance, testosterone that will not clim, acne that refuses to clear, stubborn cholesterol patterns, fat-soluble vitamin deficiencies, cold hands, morning fatigue, brain fog, the same fluid keeps appearing at the bottom of the chain. And it is not the one most people think.
Not blood. Not lymph. Bile.
I touched on bile before. This time I followed where it leads, and the web of connections is fascinating. Research from the last couple of years has made the picture even clearer. Dozens of studies have mapped how bile acids act as signaling molecules, how gut microbes reshape them into hundreds of previously unknown bile acid conjugates, how they regulate immune cells, how they drive thyroid hormone activation at the tissue level, and how modern environmental toxins, including microplastics, accumulate in human bile.
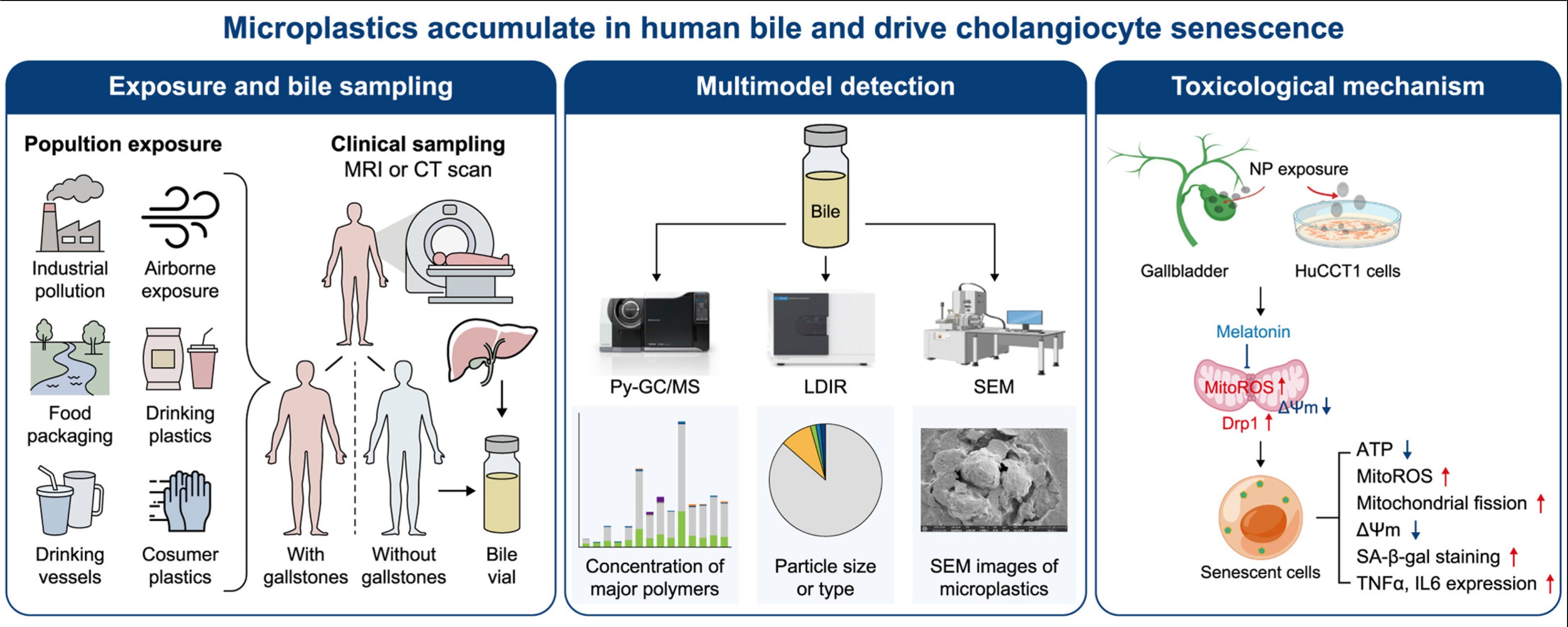
A 2026 study published in the journal Environmental Science and Ecotechnology found microplastics in every human bile sample they tested. Patients with gallstones carried roughly 3.7 times the microplastic burden of controls. The research team then showed that chronic low-dose nanoplastic exposure damages the cells lining the bile ducts through mitochondrial dysfunction and premature cellular aging.
To understand why this matters, we have to start with what bile is actually doing.
What bile actually is, and why it runs so much of your biology
Most people think of bile as a digestive juice that helps break down fat. Technically true, dramatically incomplete.
Bile is three things at once. It is a fat emulsifier. It is the body’s primary exit door for fat-soluble waste. And it is a signaling fluid, carrying molecules that talk directly to receptors on your liver, intestine, muscle, fat tissue, and immune cells.
Your liver makes about 500 to 600 ml of bile every day. Between meals, it is stored and concentrated in the gallbladder. When food arrives in the small intestine, especially food containing fat, cholecystokinin is released and the gallbladder squeezes bile into the duodenum through the common bile duct. Once its job is done in the intestine, about 95% of the bile acids are reabsorbed at the end of the small intestine and shuttled back to the liver for reuse. This loop is called enterohepatic circulation, and each bile acid molecule gets recycled roughly 20 times.
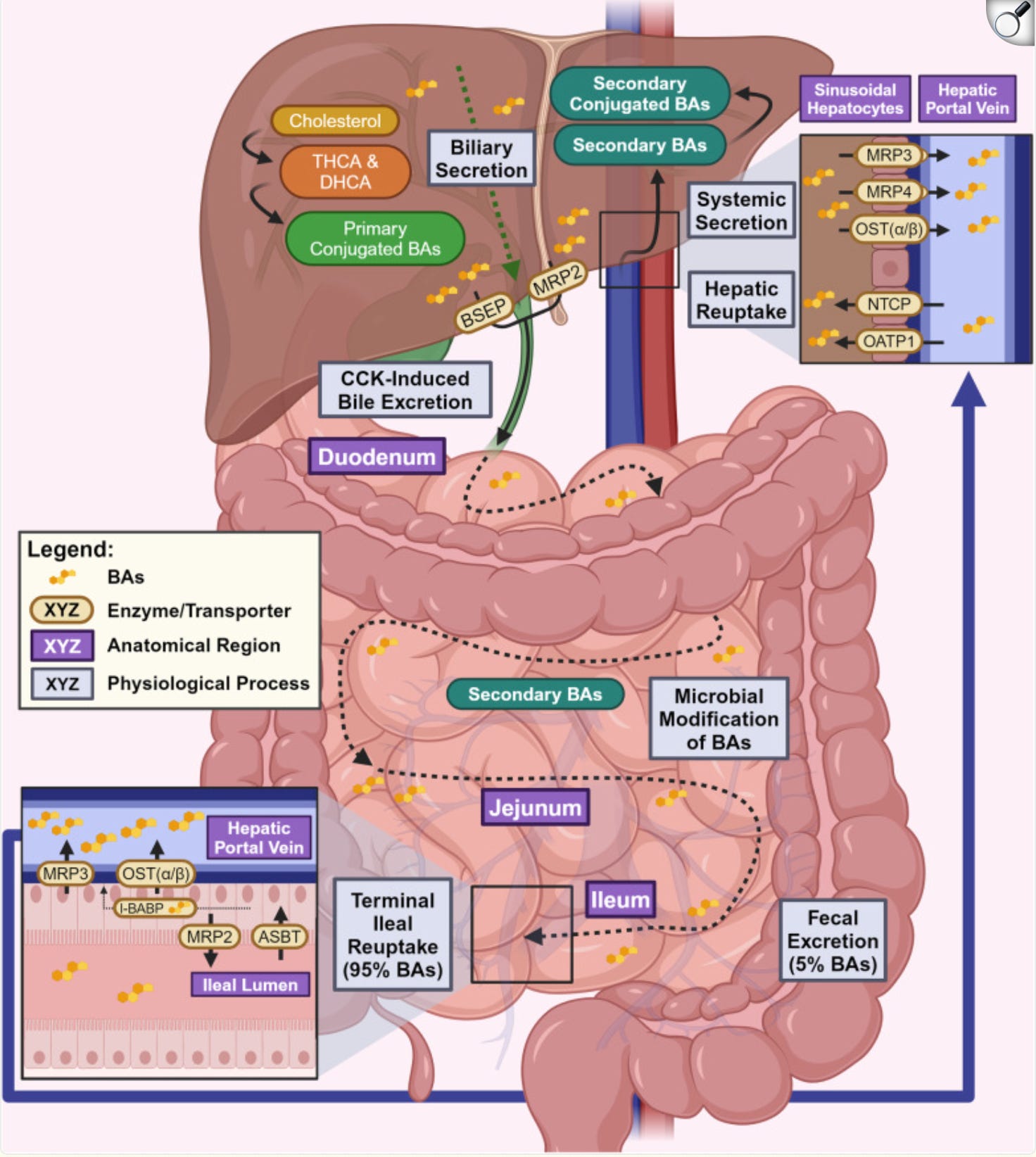
Inside bile you find bile acids made from cholesterol, phospholipids like phosphatidylcholine, cholesterol itself being excreted, bilirubin from broken-down red blood cells, conjugated hormones the liver is trying to eliminate, conjugated drugs and their metabolites, heavy metals, and fat-soluble environmental toxins.
Two exits exist for waste in the human body. The kidneys handle water-soluble waste. Bile handles fat-soluble waste. The second category is now enormous: plasticizers, bisphenols, pesticides, flame retardants, cosmetic chemicals, drug residues, mycotoxins, old hormones, cholesterol metabolites - all of them are fat-loving molecules. All of them leave through bile or do not leave.
Here is the part that changes everything: if bile does not flow properly, the waste it is supposed to carry out simply gets reabsorbed and sent back to the liver. Again. And again. The same loop that makes bile efficient makes it dangerous when the flow stalls.
The three jobs that decide how well you age
Bile runs three jobs that, taken together, are the closest thing in physiology to an aging control panel. They matter equally for men and women, and each one fails in a recognizable pattern when bile stalls.
Job one: hormone clearance, the estrogen problem and more
Hormones have a lifecycle. After a hormone is produced and used, the liver deactivates it through a two-phase process, then packages it into bile for excretion. This happens to estrogen, testosterone metabolites, cortisol metabolites, thyroid hormone metabolites, and every synthetic hormone you have ever taken.
Estrogen shows the problem most clearly because it is the most studied and because its metabolites are biologically active enough to cause real trouble when they recirculate.
Studies using radiolabeled estrogen in women found that about 65% of estradiol, 48% of estrone, and 23% of estriol end up in bile on their way to excretion. That is the majority of your circulating estrogen, routed through bile. If bile flow is compromised, so is estrogen clearance. It is that direct.
Men are not exempt from this. Men make estrogen too, produced mainly by aromatization of testosterone in adipose tissue and other peripheral sites. The same liver-bile-gut route processes it. When bile is sluggish in men, estrogen metabolites accumulate. This is one reason aging men with poor liver and bile function develop the classic pattern of rising estrogen and falling testosterone.
Three things can break this clearance, each at a different point in the loop:
• The liver does not conjugate efficiently. If Phase II conjugation is weak, estrogen leaves the liver in a form that is not properly tagged for excretion, and reabsorption is easy.
• The bile itself does not flow. Conjugated estrogen ends up stuck in the bile ducts or gallbladder, reabsorbing passively back into circulation before it even reaches the intestine.
• Gut bacteria strip the tag off in the intestine. Even if conjugation and flow work, certain gut bacteria produce an enzyme called beta-glucuronidase that cleaves the glucuronic acid off the estrogen, reactivating it. The freshly un-tagged estrogen then slips back through the gut wall and returns to the liver for another round. This microbial community that handles estrogen in the gut has its own name in the literature: the estrobolome.
Note: I covered that mechanism fully in my Low Estrogen AND Estrogen Dominant piece. What matters for this article is that slow bile makes the gut problem worse, because the longer estrogen sits in the gut, the more time bacteria have to reactivate it.

This is the mechanism behind what functional medicine calls estrogen dominance. The problem is usually not that the ovaries make too much estrogen. It is that clearance is broken at one or more of those three points, so the same pool of estrogen keeps recirculating.
The same mechanism applies to environmental estrogens, the ones from plastics and pesticides. They get conjugated, dumped into bile, and either cleared or reabsorbed depending on whether the loop is working.
Job two: detoxification, especially the fat-soluble kind
The liver detoxifies in three steps, and bile is how step three actually leaves the body.
In plain terms, step one uses a family of liver enzymes (the CYP450s) to grab hold of a toxin and make it chemically reactive. Step two attaches a water-soluble molecule, something like glucuronic acid, sulfate, glutathione, or an amino acid, which neutralizes the toxin and prepares it for export. Step three is the physical transport of the neutralized toxin out of the cell and out of the body, either through urine or through bile.
Water-soluble toxins exit via urine. Fat-soluble toxins exit via bile. And modern life is overwhelmingly fat-soluble in what it exposes you to.
Phthalates from food packaging. Bisphenols like BPA, BPS, and BPF from receipt paper and plastic-lined cans. PFAS from nonstick coatings and waterproofing. Glyphosate residues. Pesticide metabolites. Flame retardants. Mycotoxins from water-damaged buildings. Endocrine-disrupting chemicals in cosmetics and personal care. Heavy metals like mercury and cadmium. All of them, processed by the liver, dumped into bile for removal.
This is no longer abstract. As I mentioned above, recent research has directly detected microplastics inside human bile, and shown they accumulate there and drive senescence in the cells that line the bile ducts. The modern toxin load passes through bile and damages the system that moves it at the same time.
For the exit to work, all three steps must be in sync. The liver must conjugate the toxin. Bile must flow. The gut must carry the toxin out before microbial beta-glucuronidase and other microbial enzymes cleave the tag off and send it back. Break any link and you accumulate body burden.
This is the core of what I mean by detox. Not a juice cleanse. The actual, measurable, chemical process your body runs every minute to keep fat-soluble waste from building up in your tissues.
Job three: fat absorption, vitamin status, and hormone building
Bile acids lower the surface tension of dietary fats. They pull large oily droplets apart into microscopic ones, so the pancreas’s fat-digesting enzymes can actually get at them. Without bile, most dietary fat slides through undigested.
When bile flow is low, three consequences follow.
First, fat absorption drops. Pale, floating, oily stools are the textbook sign. So are foul-smelling gas and bloating after fatty meals.
Second, fat-soluble vitamin status collapses. Vitamins A, D, E, and K ride into the body on the same absorption system as fat. Without bile, they do not enter. Low vitamin D despite supplementation, low vitamin K2 showing up as early arterial calcification, low vitamin A reflected in poor night vision and skin problems, low vitamin E showing up as increased oxidative damage. These are not separate problems. They are symptoms of one broken absorption system.
Third, your ability to build steroid hormones depends on cholesterol, and cholesterol is where bile and hormones meet.
Cholesterol, bile, and why you cannot make good hormones without either
Cholesterol is a structural molecule and a hormone precursor. Every steroid hormone in your body is made from cholesterol. Pregnenolone is made directly from cholesterol by an enzyme called CYP11A1, and pregnenolone is the mother molecule from which progesterone, DHEA, testosterone, estrogen, cortisol, and aldosterone are all derived.

The same cholesterol is also the raw material for bile acids. The liver converts cholesterol into bile acids using an enzyme called CYP7A1, and this is the single largest route your body uses to dispose of cholesterol.
So cholesterol sits at a fork. Part of it gets pulled into steroidogenesis, becoming the hormones that run your biology. Part of it gets pulled into bile acid synthesis, becoming the detergents and signaling molecules that keep bile flowing.
Both routes compete for the same pool, and both depend on thyroid hormone to run at a good pace.
Thyroid hormone, specifically T3, drives the conversion of cholesterol into both progesterone and bile acids. The liver needs T3 to run these conversions efficiently. When thyroid function is low, both conversions slow down, and cholesterol tends to accumulate in the blood because it is not being moved through either pathway. This is why hypothyroid patients frequently run high cholesterol, and why guidelines recommend checking thyroid before starting statin therapy. Treating the thyroid often normalizes cholesterol on its own.

Bile flow itself also regulates cholesterol clearance. Impaired bile acid synthesis and impaired bile flow cause cholesterol to back up in the blood because it cannot leave through the bile acid pathway. This is part of why hypothyroid people get cholesterol gallstones at higher rates. When bile contains too much cholesterol relative to bile acids, the cholesterol crystallizes into sludge and stones.
So far, the picture is one of pileup. But the pileup is only half the story.
The other side of the fork is supply. Since cholesterol is also the raw material for every steroid hormone in the body - pregnenolone, progesterone, DHEA, testosterone, estrogen, cortisol, aldosterone - if you eat a very low-fat diet for years, or your body is not absorbing fat well because of weak bile, or chronic stress is burning through cholesterol faster than it can be made, cholesterol supply runs thin. In that scenario, the usual pileup from bile sluggishness can be masked or even reversed by the shortage on the input side.
This is why cholesterol number alone tells you almost nothing about bile status. The same bile problem can present as high cholesterol in one person (pileup dominates) or low cholesterol in another (poor input dominates). What matters is not the number, but the flow. Cholesterol should be coming in, being used for hormones and bile acids, and being cycled through. Either end of the number range, very high or very low, usually signals that the traffic has stopped moving somewhere.
The common reading, that low cholesterol is always good, collides with this biology. Cholesterol below 160 mg/dL is not a sign of health. It is a sign that the raw material for hormone synthesis is running thin, usually because thyroid, fat intake, or bile absorption is compromised. A review of those three is where the answer usually lives.
Bile and cholesterol are locked together. You need enough cholesterol to make hormones and bile acids. You need enough bile acids to absorb the fat you need to make cholesterol. And you need thyroid hormone to run both sides of this loop. Breaking any link breaks the others.
The thyroid-bile loop
There is one piece of physiology that locks bile so tightly into the bioenergetic framework that you cannot separate them.
Bile acids do more than emulsify fat. They activate two receptors called FXR and TGR5, and TGR5 does something remarkable in tissues that burn a lot of energy.
In brown adipose tissue and skeletal muscle, bile acids activate TGR5, which induces an enzyme called deiodinase 2 (DIO2). DIO2 converts inactive T4 into active T3 locally in those tissues, increasing mitochondrial energy expenditure. This happens without necessarily changing blood levels of T3. Good bile flow amplifies thyroid signaling at the tissue level.
Now close the loop from the other direction. T3 increases the conversion of cholesterol into bile acids, and T4 is a strong relaxant of the sphincter of Oddi, the muscular gate that controls bile flow out of the common bile duct. In hypothyroid people, the sphincter is tighter. Gallbladder motility slows. Bile pools. Cholesterol saturation in bile rises. And gallstones form at much higher rates. Subclinical hypothyroidism is found in a significant fraction of gallstone patients.
So the loop runs like this. Bad thyroid creates sluggish bile. Sluggish bile means less local T3 in muscle and brown fat, because TGR5 is not being activated properly. Less local T3 means lower energy expenditure and further worsening of every metabolic consequence of low thyroid, including the bile itself.
This is the loop that traps a lot of people. Treating thyroid in isolation leaves half of it broken. Treating bile in isolation without adequate thyroid support gives you incomplete flow.
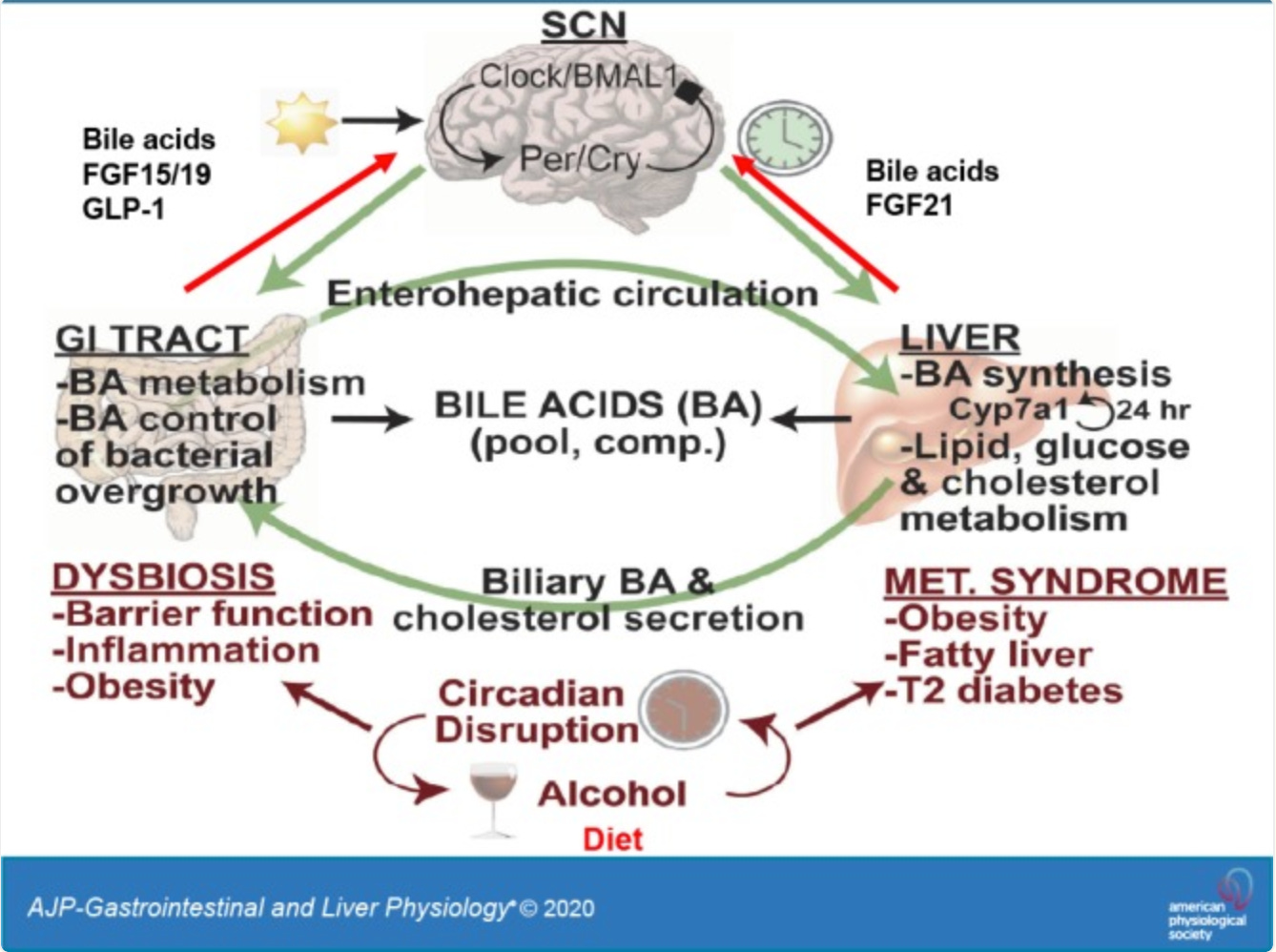
The wider picture: bile is also a metabolic regulator
The three jobs above are what most people feel first. But bile acids also act as signaling molecules across the whole body, talking to receptors on the liver, intestine, fat, muscle, and immune cells. A 2024 review in Signal Transduction and Targeted Therapy laid out how disrupted bile acid signaling shows up in conditions that, on the surface, have nothing to do with bile:
Blood sugar and insulin resistance. Bile acid signaling through FXR and TGR5 increases insulin sensitivity and reduces how much glucose the liver dumps into the bloodstream. Sluggish bile contributes to fatty liver and type 2 diabetes.
Appetite and satiety. Bile acids stimulate FGF19, which reaches the hypothalamus and suppresses hunger neurons. Healthy bile flow is part of how the body knows it is fed.
Systemic inflammation. FXR activation blocks the NLRP3 inflammasome and inhibits NF-κB, two of the main drivers of chronic low-grade inflammation. Weak bile signaling means the brake on inflammation fails.
Cardiometabolic disease. Fatty liver, NASH, atherosclerosis, type 2 diabetes, and obesity all share disrupted bile acid signaling as a contributing mechanism.
Why modern humans are uniquely vulnerable to bile stagnation
Bile stagnation is not a rare disease. It is an epidemic in everything but name. The combination of modern diet, environment, stress, and pharmaceutical exposure puts pressure on the bile system from every angle.
Women have a structural predisposition. Estrogen slows bile acid uptake into hepatocytes, pregnancy transiently slows bile flow (which is why some women develop cholestasis of pregnancy), and every year of hormonal contraception loads the liver with synthetic estrogens and progestins that need to be processed and excreted. Studies have documented impaired bile flow and altered bile composition in women on oral contraceptives.
Men are not off the hook. Men are more likely to be exposed to occupational toxins, to drink alcohol at higher rates, and to run their liver harder for longer before symptoms appear.
Layered on top of sex-specific factors, the modern lifestyle creates conditions that reliably break bile flow:
· Processed food and fast food as the daily norm. Industrial seed oils, refined sugars, emulsifiers, preservatives, and additives in packaged and restaurant food all push the liver hard. Seed oils in particular (soybean, corn, sunflower, safflower, grapeseed, canola, cottonseed) oxidize easily, increase oxidative stress in the liver, and alter bile composition. This is the single biggest driver of bile and liver dysfunction in the general population.
· Sedentary lifestyle. Physical movement directly supports gut motility, gallbladder contraction, and venous return to the liver. Sitting for most of the day slows all of it. Bile sits longer, transit slows, and the whole enterohepatic loop becomes sluggish.
· Obesity and fatty liver. Non-alcoholic fatty liver disease, now affecting roughly 25% of the global population, alters bile acid synthesis, impairs bile flow, and shifts the bile acid pool toward more damaging, less functional forms. Fatty liver and sluggish bile feed each other.
· Chronic stress and high cortisol. Suppress thyroid conversion, slow gut motility, and reduce bile flow.
· Alcohol. Even moderate regular drinking diverts the liver from hormone and toxin clearance work and damages bile duct cells directly over time.
· Endotoxin load from gut dysbiosis. Forces the liver to burn capacity handling bacterial toxins, leaving less for hormone and xenobiotic clearance. Processed food reliably produce this pattern.
· Hormonal medications. The combined oral contraceptive pill (containing ethinyl estradiol and a progestin) is a well-documented cause of altered bile composition and increased cholestasis risk. Oral conjugated equine estrogens (such as Premarin) and oral estradiol go directly to the liver via first-pass metabolism, which loads it heavily. (Transdermal estradiol bypasses this first-pass step and does not significantly burden bile flow or composition). Prescriptions that can cause cholestasis or heavy biliary excretion include certain antibiotics (amoxicillin-clavulanate, erythromycin, flucloxacillin), anabolic and 17-alkylated steroids, some antiepileptics, azathioprine, and chlorpromazine.
· Environmental toxin load. Plastics, pesticides, phthalates in scented products, flame retardants, PFAS in waterproof coatings. All fat-soluble. All heading for bile.
· Low-fat dieting. Less common in the general population but extremely common among health-conscious women. Without a fat signal at a meal, cholecystokinin does not release strongly, the gallbladder does not fully contract, and bile sits and thickens.
· Fasting and skipping meals. Prolonged fasting leaves bile concentrated in the gallbladder for hours with no discharge. This is the documented mechanism behind the rise in gallstones during rapid weight loss and during long intermittent fasting protocols.
Two opposite dietary patterns damage bile. On one side, the Standard American Diet of processed food and seed oils. On the other, restrictive protocols that go too far in the other direction: long-term low-fat dieting, long fasts, and anti-fat cleanses. Both produce the same end result.
How sluggish bile shows up
The obvious signs are easy to list. What is harder is recognizing the quieter ones, because they are what sends people on years of specialist visits without anyone connecting the dots.
Digestive signs
Bloating 30 to 60 minutes after eating fat. Discomfort or a dull ache under the right rib. Nausea after fatty meals. Pale, clay-colored, floating, or oily stools. Constipation that alternates with looser stools. Burping that tastes sulfurous. Fat intolerance that gets worse over time.
Hormonal signs in women
PMS that intensifies year over year. Heavy or painful periods. Breast tenderness. Irregular cycles. Fibrocystic breasts. Estrogen dominance symptoms despite normal estrogen on lab tests. Low progesterone that does not respond well to supplementation. Early perimenopause symptoms.
Hormonal signs in men
Low morning testosterone. Rising estrogen or estrone on hormonal panels. Gynecomastia that appears with age. Erectile dysfunction not explained by cardiovascular or psychological factors. Poor recovery from training. Accumulating abdominal fat despite diet and exercise.
Skin signs
Jawline and chin acne, especially cyclical in women. Rosacea. Itchy skin without a rash, especially at night. Cherry angiomas appearing in clusters. Pigmentation changes. Slow wound healing.
Metabolic and energy signs
Cold hands and feet. Morning temperature below about 97.8°F (36.5°C). Energy crashes after fatty meals. Brain fog that correlates with digestive upset. Difficulty losing fat.
Lab clues
There is no single test that says “your bile is stuck.” What exists is a pattern. Some of the most useful markers:
• GGT creeping up, even inside the reference range. GGT is one of the most sensitive markers of early bile duct stress and is often elevated before anything else.
• ALP elevated, especially when paired with elevated GGT. The combination points to a cholestatic pattern. ALP alone can be elevated from bone turnover, so pairing it with GGT clarifies the source.
• Direct (conjugated) bilirubin may be elevated in more advanced cholestasis. Early or mild bile stagnation often leaves bilirubin normal. It is not a sensitive early marker.
• Elevated estrogen metabolites on DUTCH or similar hormone metabolite testing, especially with low progesterone to estrogen ratio.

• Hs-CRP elevated. Low-grade inflammation markers. Chronic inflammation stresses the liver and contributes to bile acid pool changes. Not specific to bile but often part of the pattern.
• Low HDL. Associated with cholestasis and liver dysfunction. HDL metabolism runs through the liver, and when liver is stressed, HDL often drops.
Three or four of these in combination, with the digestive pattern, is usually enough to start investigating bile as the upstream issue.
Why nobody tests for this
Three reasons. First, there is no single lab marker for bile stagnation. Reading the pattern requires integrating several markers and symptoms, which modern specialized medicine is not organized to do.
Second, there is no blockbuster drug. Ursodeoxycholic acid exists for primary biliary cholangitis, an autoimmune bile duct disease. But the everyday stagnant-bile physiology that wrecks health in millions of people has no pharmaceutical target, because it cannot be packaged as a diagnosis and sold as a pill.
Third, bile does not fit inside any one specialty. It sits upstream of skin, hormones, gut, and metabolism. It explains too many symptoms at once, which in modern medicine is a reason to ignore something, not investigate it.
The protocol
Below is the protocol I have refined over years of personal experimentation, study, and adjustment. Every supplement, food, and sequencing decision was tested before it made it into this version. It is built around mechanism and sequenced to match the order your body actually needs: calm the system, fuel it, stimulate flow, then catch what flow releases.