
Your Posture Problem Is a Metabolism Problem
Why modern posture advice often makes things worse, and what your body actually needs to hold itself up


Good posture is a direct reflection of your health. It signals the state of your metabolism, your nervous system, your hormonal balance. But it’s also something beyond health. It’s grace. It’s presence. It’s the quiet authority you carry when you walk into a room before you’ve said a single word. People feel it. They don’t analyze your spinal curvature or measure your scapular protraction. They feel that this person is vital, composed, and grounded. That impression is built entirely on how your body organizes itself in space. And you can’t fake it. You can’t perform presence. It either lives in your body or it doesn’t.
I started ballet as a young girl. If you know anything about Russian classical ballet training or Vaganova method, you know it’s one of the most rigorous systems of postural education ever developed. Every class began with “placement,” the setting of the body. Spine vertical. Head high. Shoulders down and open. The barre work, the pliés, the relevés, the slow fondus, all of it was designed to train the deep stabilizing muscles through sustained, low-intensity, proprioceptive-rich repetition. Before you were allowed to do anything complex, your body had to learn how to hold itself. Years were spent on this.
It gave me things I still carry. A deep internal sense of where my body is in space. An understanding of how the head organizes the entire postural chain. The ability to feel when a muscle is gripping versus when it’s actually working. These aren’t things you learn from a YouTube video or a posture corrector. They come from years of training the nervous system, slowly, at the barre, with a teacher who corrected you by touch.
But ballet also gave me problems. The forced turnout created compensatory tension in my lumbar spine. The aesthetic demand for a perfectly held, hyper-extended thorax pushed my body past what the tonic system naturally produces into a performance posture that looks gorgeous on stage but creates compression everywhere else. The culture of pushing through pain taught me to override signals my body was sending for good reason. I spent years after ballet unraveling patterns that the training had installed, learning the difference between a posture that looks right and a posture that feels right from the inside.
That dual experience is what eventually led me to study muscle physiology extensively. And it’s what makes me say, with confidence built on both research and lived experience: almost everything you’ve been told about posture is either incomplete or actively harmful.
Watch any toddler and you’ll see what healthy posture looks like. Spine long. Squat deep with a perfectly neutral pelvis. No one coached them. Their nervous system organized their posture automatically, because the conditions for automatic posture were intact.
So what happened?
The standard answer is that modern life ruined us. Sitting, screens, sedentary jobs. And those things matter, but they’re surface-level explanations. The deeper story is about what’s happening inside your body that makes your postural system stop working the way it was designed to. That story involves your muscles, your fascia, your nervous system, your hormones, and your cellular metabolism. And almost none of the conventional posture advice addresses any of it.
In fact, most of it makes things worse.
This article is going to walk through the real anatomy and physiology of postural control, explain why the most popular corrections are counterproductive, and give you a framework for actually restoring the kind of effortless uprightness that doesn’t require constant vigilance.
Part 1: The Two Muscle Systems
Your body has two fundamentally different muscle systems. Understanding this distinction is the key to understanding why most posture advice fails.
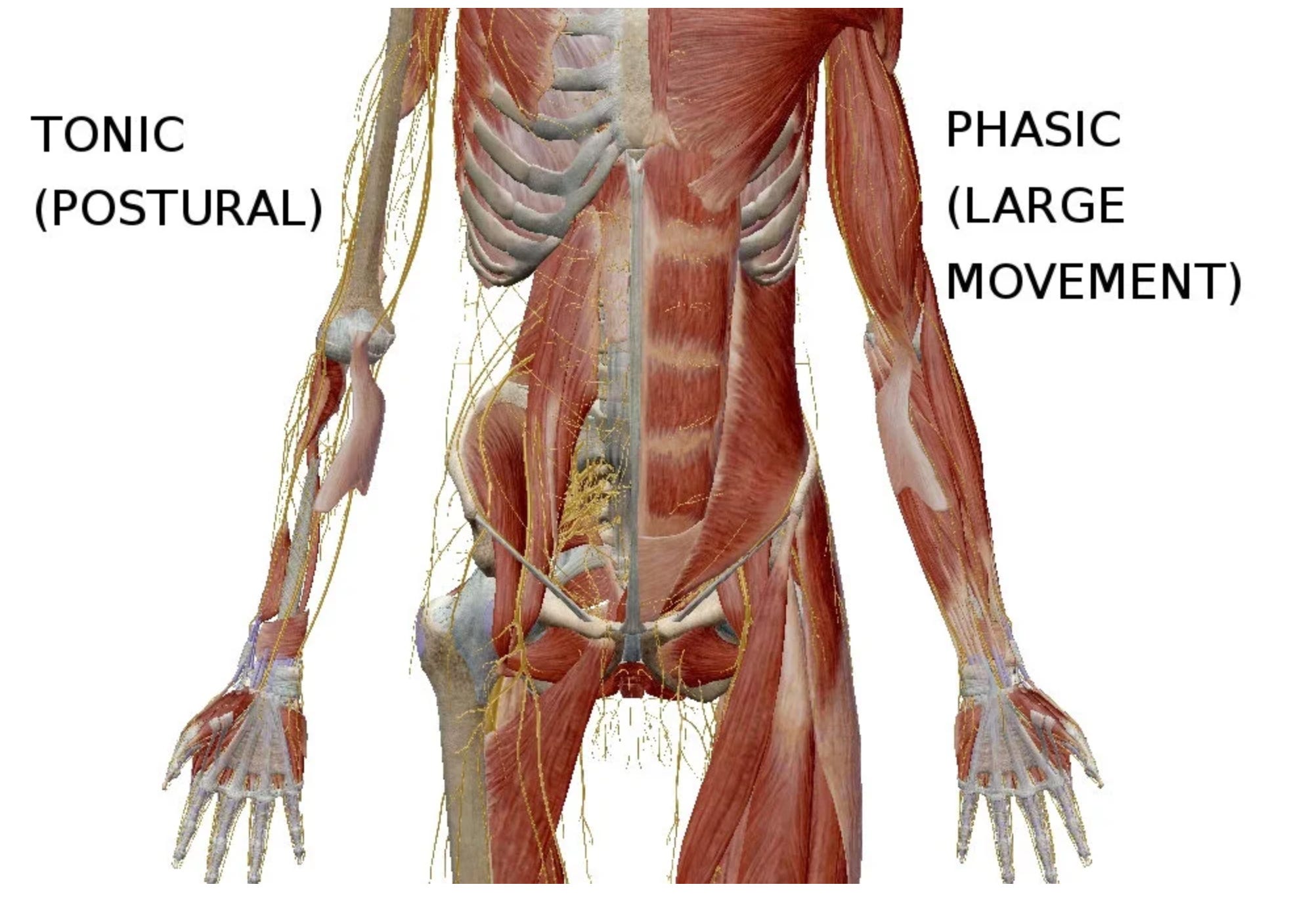
Tonic muscles are your deep stabilizers. They sit close to the bone, close to the joint. They’re composed predominantly of Type I (slow-twitch) fibers, built for sustained, low-level contraction. They don’t produce big movements. They produce stability. They’re always on to some degree, maintaining a low-grade background contraction that keeps your skeleton organized against gravity. You don’t consciously activate them. They fire reflexively, governed by proprioceptive feedback loops that operate below conscious awareness.
This is what classical ballet barre work actually trains, even if most ballet teachers wouldn’t describe it in these terms. The slow pliés, the sustained relevés, the controlled fondus at the barre are all low-intensity, sustained contractions that recruit Type I fibers in the deep postural muscles. The reason ballet dancers have such distinctive carriage isn’t because they voluntarily hold themselves up. It’s because years of barre work have trained their tonic system to do it automatically. The barre is the most sophisticated tonic muscle training protocol ever developed. It just wasn’t designed with that language.
The key tonic muscles for posture include the multifidus (the deep spinal stabilizer that spans 2-4 vertebrae and controls segmental motion), the transversus abdominis (the deepest abdominal muscle that acts like a corset around the trunk), the deep cervical flexors (which stabilize the neck from the front), the soleus (the primary anti-gravity muscle of the lower leg), and the diaphragm (which is both a respiratory and a postural muscle, a dual role that becomes critically important later).
Phasic muscles are your movers. They’re composed predominantly of Type II (fast-twitch) fibers, designed for powerful, rapid contractions. They produce force, speed, and big movements. They fire on demand and then shut off. Think biceps, rectus abdominis (the “six-pack”), upper trapezius, hamstrings, pectorals.
Here is the problem. When tonic muscles underperform, phasic muscles try to compensate. They take over stabilization duties and because phasic muscles fatigue quickly and produce crude, large-scale contractions instead of the fine-tuned segmental control that tonic muscles provide, the result is a body held together by bracing and gripping rather than by true stability.
This is the state most adults live in.
The upper trapezius clamps down to try to stabilize the head and neck because the deep cervical flexors have gone quiet. The rectus abdominis grips the front of the trunk because the transversus abdominis has lost its reflexive activation. The erector spinae locks into a global contraction along the entire back because the multifidus has atrophied at specific vertebral segments.
The person feels “tight” everywhere. Their muscles ache. They feel stiff in the morning. They can’t relax even when they lie down. And every bit of conventional posture advice they follow reinforces this pattern, because conventional posture advice is built entirely around activating phasic muscles.
“Squeeze your shoulder blades together.” That’s the rhomboids and middle trapezius. Phasic muscles.
“Engage your core.” That’s typically the rectus abdominis and external obliques. Phasic muscles.
“Tuck your chin.” Done as a voluntary effort, that’s the sternocleidomastoid. Phasic.
Each of these cues creates a voluntary contraction in a movement muscle, layered on top of a system that’s already stuck in compensatory bracing. You’re adding tension to a system that needs less tension, not more.
To appreciate the scale of what’s involved: approximately 300 muscles participate in establishing and maintaining upright posture. Around 150 of those support the spinal column alone, and about 20 muscles work just to balance the head on the neck. The idea that you can manage this system by consciously squeezing two or three muscle groups is like trying to conduct an orchestra by playing the drums louder.
Part 2: The Multifidus
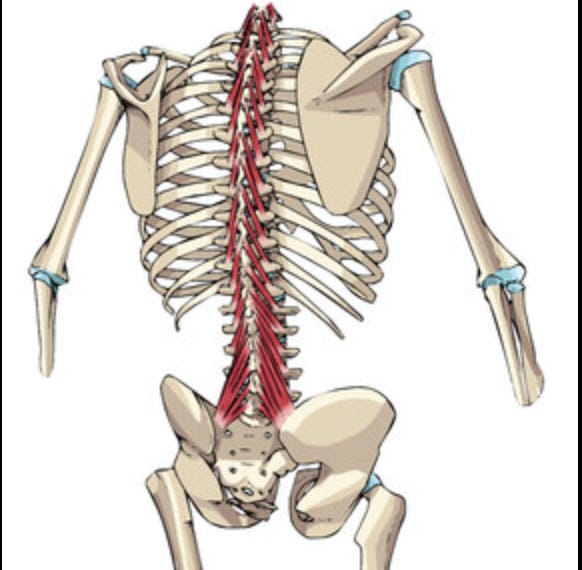
If there’s one muscle that tells the story of postural dysfunction, it’s the multifidus. This is a deep spinal muscle that runs along the entire length of your vertebral column, most developed in the lumbar region. Its fascicles attach from the spinous process to the mamillary processes, iliac crest, and sacrum, spanning 2 to 5 vertebral segments.
The multifidus has the largest cross-sectional area of any muscle in the lumbar spine. It produces segmental stabilization, meaning it controls the position and movement of individual vertebrae relative to each other. When the multifidus is functioning properly, each vertebra is stabilized during movement, so the forces traveling through your spine are distributed evenly across segments.
It’s composed primarily of Type I fibers, making it fatigue-resistant and suited for sustained postural work. And it contains an exceptionally high density of muscle spindles, the proprioceptive sensors that tell your brain where your spine is in space. The multifidus is as much a sensory organ as it is a motor one.
Here’s what happens when it fails.
Research consistently shows that people with low back pain have multifidus atrophy, particularly at the level of the affected vertebra. The muscle loses cross-sectional area. Fat infiltrates the muscle tissue, replacing contractile fibers with non-functional tissue. And critically, the timing of activation changes. In a healthy spine, the multifidus pre-activates before limb movement, stabilizing the spine in anticipation of the load. In people with back pain, this anticipatory activation is delayed or absent.
The deeper problem is that the multifidus doesn’t spontaneously recover, even after the pain resolves. Studies have shown that without specific intervention, lumbar multifidus remains atrophied after acute episodes of low back pain. The nervous system essentially “forgets” how to activate it. The global muscles (erector spinae, rectus abdominis) take over, and the system never resets.
Now consider what conventional posture advice does here. ‘Strengthen your back’ usually means exercises like heavy back extensions and deadlifts, which predominantly recruit the erector spinae, the global extensor. These exercises matter, and I’ve written before about the importance of training the spinal extensors for anti-aging and structural strength. The problem is when they’re prescribed as posture fixes. These exercises primarily load the outer layer, the erector spinae, which produces global extension force. The multifidus, the deeper segmental stabilizer, gets some work during compound lifts, especially during bird dogs and anti-rotation exercises. But if the multifidus has already atrophied and lost its reflexive activation pattern, which happens after back pain episodes or prolonged inactivity, heavy compound exercises alone won't restore it. The erector spinae just compensates harder. You get a strong back that can move heavy loads but still can't control individual vertebrae during quiet standing.
Even worse, the rotatores muscles, the deepest layer of the transversospinales group (deeper than multifidus), have a cross-sectional area so small they can barely produce meaningful force. Their value lies elsewhere. The rotatores contain five to seven times the density of muscle spindles compared to multifidus and semispinalis. These tiny muscles are essentially proprioceptive organs. They exist to sense position, not to produce movement. When they atrophy or become inhibited, you lose spinal position sense. Your brain literally doesn’t know where your vertebrae are.
This is why people with chronic back problems often report feeling “unstable” or “out of alignment” even when imaging shows nothing structurally wrong. Their proprioceptive system has degraded. They’ve lost the internal GPS of their spine.
Part 3: The Diaphragm Is a Postural Muscle
Most people think of the diaphragm as a breathing muscle. It is. But it’s equally a postural muscle, and this dual role creates one of the most important and most overlooked dynamics in the entire postural system.
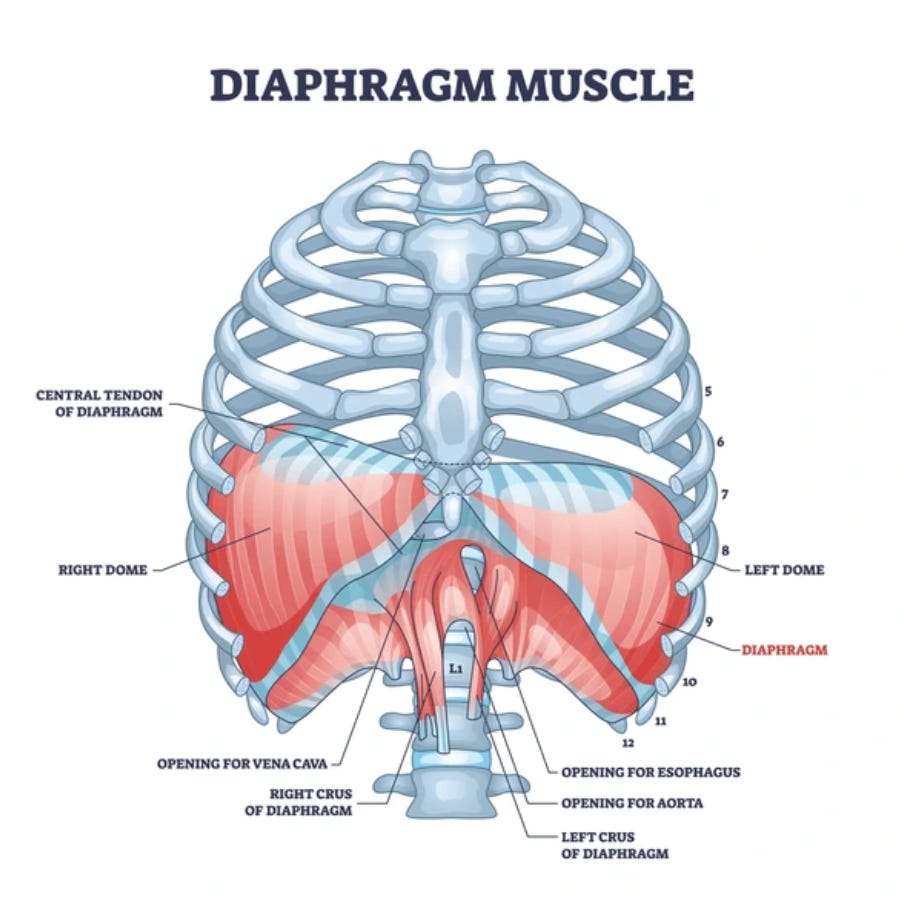
The diaphragm sits at the base of the thoracic cavity, doming up under the ribs. When it contracts during inhalation, it descends into the abdominal cavity, creating negative pressure in the chest (pulling air in) and positive pressure in the abdomen (pushing the organs down and out). This increase in intra-abdominal pressure (IAP) is one of the primary mechanisms of lumbar spine stabilization.
Think of the trunk as a cylinder. The diaphragm is the top. The pelvic floor is the bottom. The transversus abdominis wraps around the sides. When all three contract in coordination, they create a pressurized column that supports the lumbar spine from inside. This is real core stability. It’s hydraulic, not muscular in the traditional sense.
Research by Kolar and colleagues using MRI synchronized with spirometry showed that during postural tasks, the diaphragm descends further into the abdominal cavity than it does during quiet breathing. When the demands on stability increase, the diaphragm increases its postural contribution. This is an automatic process governed by the nervous system. You don’t decide to do it.
But here’s where it breaks down.
The body will always prioritize breathing over stabilization. If your breathing pattern is dysfunctional, if you’re a chest breather, a mouth breather, or a chronic hyperventilator, the diaphragm can’t perform both of its jobs simultaneously. The respiratory demand wins, and postural support is sacrificed.
The accessory breathing muscles (scalenes, sternocleidomastoid, upper trapezius, pectoralis minor) take over respiratory duties. These are all muscles of the neck, chest, and upper back. When they’re chronically recruited for breathing, they become tight and overactive, pulling the head forward, rounding the shoulders, and elevating the ribcage into a fixed position of inhalation.
This is the anatomical basis of the classic “forward head, rounded shoulder” posture that physiotherapists spend so much time trying to correct with stretches and strengthening exercises. They’re treating the downstream compensation without addressing the upstream cause: dysfunctional breathing has hijacked the postural system.
The diaphragm can’t stabilize the spine if it’s not descending properly. The transversus abdominis can’t generate appropriate fascial tension if the diaphragm isn’t creating sufficient IAP. The pelvic floor can’t maintain its tone if the pressure dynamics of the abdominal cylinder are disrupted. The entire system cascades.
So when someone tells you to “pull your shoulders back” to fix your rounded posture, they’re asking you to override with voluntary effort what is actually a respiratory and pressure problem. You can retract your shoulders all day long. If your diaphragm isn’t descending properly during breathing, those shoulders will round forward again the moment you stop thinking about it.
Part 4: Fascia, Tensegrity, and Why You Can’t Correct Posture One Body Part at a Time
Your body is not a stack of blocks. It’s a tensegrity structure.

Tensegrity (tensional integrity) is a structural principle where stability comes from a continuous network of tension elements (cables) interspersed with discontinuous compression elements (struts). In your body, the fascia, muscles, tendons, and ligaments form the continuous tension network. The bones are the compression elements. They don’t stack on top of each other like bricks. They float within a web of tension.
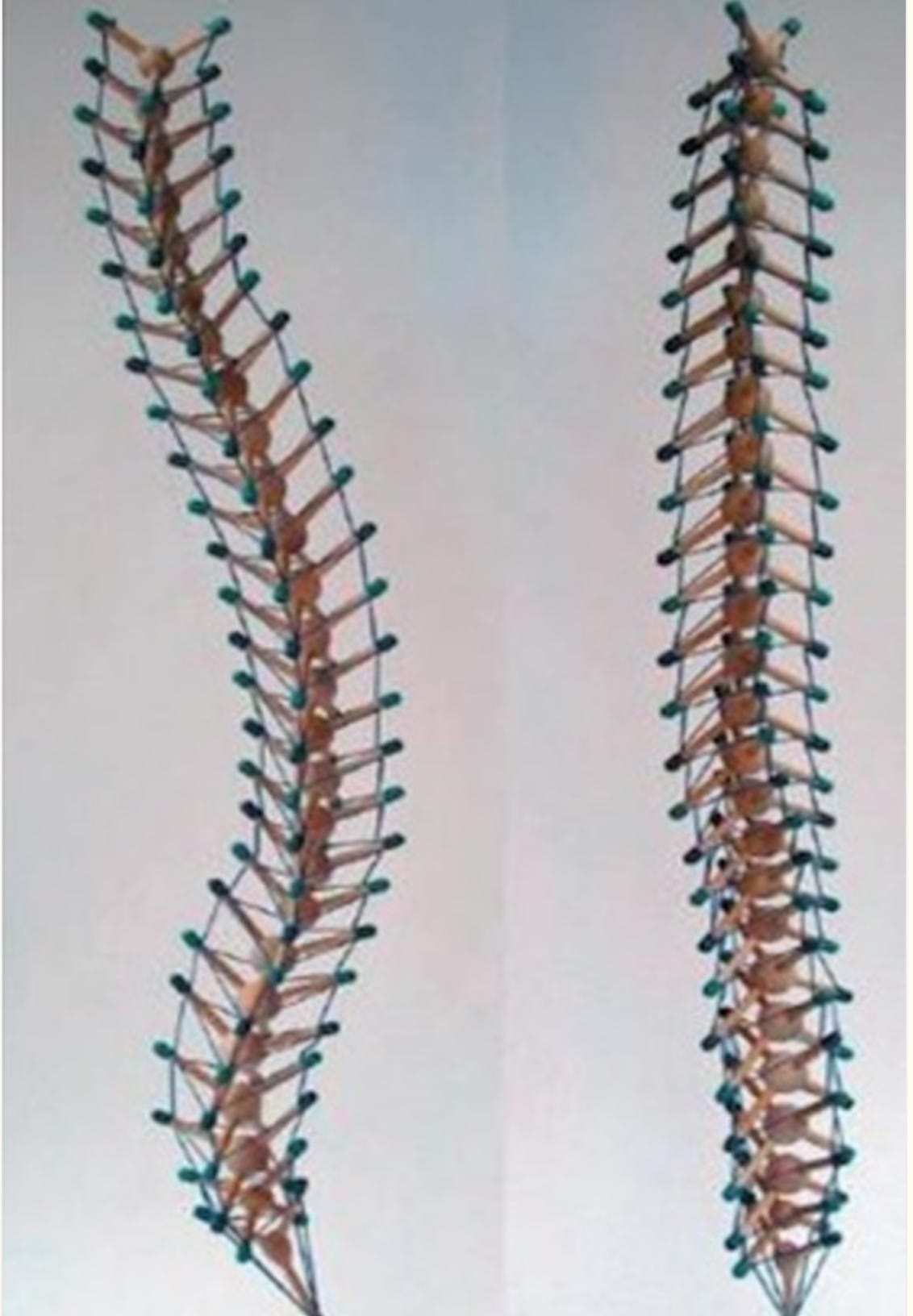
This has profound implications for posture.
In a tensegrity system, a change in tension anywhere affects tension everywhere. Pull one strand tighter, and the entire structure reorganizes. This is why you can’t “fix” posture by working on one area. The person with forward head posture doesn’t just have a neck problem. They have a whole-body tension distribution problem. Their fascial system has reorganized globally around the pattern.
Fascia is a continuous connective tissue that wraps, separates, connects, and supports every structure in your body, from individual muscle fibers to entire organ systems. It contains contractile cells (myofibroblasts) that can actively change tissue tension. It contains more sensory receptors than muscle tissue, approximately ten times more, making it one of the richest sensory organs in the body. And its mechanical behavior is profoundly influenced by hydration.
Dehydrated fascia stiffens. It loses its ability to slide, glide, and transmit force smoothly. The mechanical stiffness of connective tissue depends primarily on water and fluid content, even before the contraction of fibroblasts becomes relevant. This means that basic hydration status, inflammatory state, and metabolic health directly affect fascial pliability and, by extension, postural adaptability.
The concept of myofascial chains describes continuous lines of fascial and muscular connection that transmit force across multiple joints and body regions. The superficial back line, for example, runs from the plantar fascia on the bottom of the foot, up through the gastrocnemius, hamstrings, sacrotuberous ligament, erector spinae, and up to the galea aponeurotica (the fascial sheet over the skull).
When the plantar fascia is stiff and restricted, it increases tension in the gastrocnemius and hamstrings, which tilts the pelvis posteriorly, which flattens the lumbar curve, which increases thoracic kyphosis, which pushes the head forward. The “forward head posture” originated at the foot, not at the neck.
This is why cervical retractions and chin tucks (the standard physical therapy prescription for forward head posture) often fail. They address the end of the chain while ignoring the source. And because the fascial system adapts to sustained tension by laying down more collagen in the direction of strain, the correction has to include the entire line of tension, not just the symptomatic segment.
This is also why isolated stretching often fails. Stretching one muscle in a myofascial chain doesn’t release the chain. The fascia itself needs to be addressed through sustained pressure, movement variability, hydration, and metabolic support. Fascia changes on a different timescale than muscle. It responds to slow, sustained mechanical input over minutes to hours, not to the rapid stretch-hold-release protocols that most people use.
Part 5: The Metabolic Foundation of Posture
Here is where the story goes deeper than biomechanics. Your muscles need energy to hold you up. Specifically, your tonic postural muscles need a continuous supply of ATP to maintain the sustained, low-level contractions that keep your skeleton organized against gravity.
This is where thyroid function enters the picture.
Thyroid hormone (T3) is the primary regulator of mitochondrial ATP production in skeletal muscle. T3 drives the expression of SERCA (the sarcoplasmic reticulum calcium ATPase), which is the pump responsible for recycling calcium back into the sarcoplasmic reticulum after each contraction cycle. The contraction-relaxation cycle in skeletal muscle is fundamentally a calcium cycle, and every iteration of that cycle consumes ATP.
In a hypothyroid state, SERCA expression decreases. Calcium handling becomes sluggish. Contraction-relaxation cycles slow down. Muscles become simultaneously weak and stiff, a paradox that makes clinical sense once you understand the mechanism: the muscle can contract, but it can’t efficiently relax, because relaxation is an active, energy-dependent process that requires ATP to pump calcium back into the SR.
This is why hypothyroid patients commonly present with muscle weakness, stiffness, and myalgia. Hypothyroid myopathy is estimated to affect 30 to 80 percent of hypothyroid individuals. The proximal muscles (thighs, hips, shoulders) are most commonly affected, and these are exactly the muscle groups most important for postural support.
T3 also regulates the Na+/K+-ATPase in skeletal muscle. This enzyme maintains the electrochemical gradients across the muscle cell membrane that allow proper nerve signal transmission and muscle excitability. In hypothyroid states, Na+/K+-ATPase expression decreases significantly, particularly the alpha-2 and beta-2 isoforms, which are the predominant forms in skeletal muscle. The result is altered membrane excitability, reduced nerve-to-muscle signal transmission, and further degradation of the fine motor control that postural muscles depend on.
Think about what this means practically. Your tonic postural muscles need continuous ATP production to maintain background tone. They need functional SERCA to cycle calcium smoothly. They need functional Na+/K+-ATPase to maintain membrane excitability. All three are directly regulated by thyroid hormone. When thyroid function is suppressed, even subclinically, the energy supply to the postural system diminishes. The muscles don’t fail dramatically. They fail quietly. Tone drops. Reflexive activation becomes sluggish. The body sags.
And you can do all the posture exercises you want. You can tape your back, buy the standing desk, set hourly reminders to sit up straight. If the metabolic engine driving your postural muscles is underfueled, none of it will hold.
This extends beyond thyroid. Blood sugar stability matters because the brain and nervous system are glucose-dependent, and postural control is centrally mediated. When blood sugar drops, the nervous system downregulates non-essential functions. Postural tone is one of the first things to go. Carbon dioxide levels matter because CO2 facilitates oxygen delivery to tissues through the Bohr effect. Chronic hyperventilation (common in stressed, anxious individuals) blows off CO2, reducing oxygen delivery to postural muscles and shifting the nervous system toward sympathetic dominance. Calcium and magnesium balance matters because muscle contraction requires calcium and muscle relaxation requires magnesium, and the interplay between these minerals determines the quality of muscle tone: smooth and sustained versus jerky and crampy.
The person who undereats, skips meals, runs on caffeine, sleeps poorly, and lives in a state of chronic low-grade stress has systematically degraded every metabolic input their postural system needs. No amount of corrective exercise can compensate for that.
Part 6: The Stress-Posture Feedback Loop
Stress creates a recognizable postural signature. Rounded shoulders. Head forward. Chest collapsed. Upper back curved. Jaw clenched. Shallow breathing.
This is the flexion response. It’s a protective pattern, the same one animals adopt when threatened. The ventral (front) surface of the body closes down to protect the vital organs. The extensors along the back lose tone. The body makes itself smaller, less exposed, less vulnerable.
This pattern is driven by the sympathetic nervous system and mediated by cortisol and adrenaline. Research has shown that the reticulospinal pathways, which influence background muscle tone, are directly linked to the autonomic nervous system. The same neural circuits that manage the stress response also regulate postural tone. When the sympathetic system is dominant, it biases the body toward flexion.
Studies confirm the bidirectional nature of this relationship. Upright posture during stressful tasks has been associated with lower cortisol levels and greater emotional resilience. Slumped posture has been associated with increased chromogranin A (a marker of sympathetic nervous activity) and decreased parasympathetic tone. The posture and the stress state reinforce each other in a loop.
Chronic stress, whether psychological (work pressure, relationship strain, financial worry) or metabolic (undereating, overexercising, gut inflammation, poor sleep), keeps the body in this flexion-dominant pattern. The hip flexors shorten. The thoracic spine rounds. The suboccipital muscles at the base of the skull tighten to keep the eyes level despite the forward head position, creating tension headaches and neck pain.
Here is the key insight: this pattern is chemically driven. It’s an expression of your hormonal and nervous system state. You can’t voluntarily extend a body that is chemically locked into flexion any more than you can voluntarily lower your heart rate during a panic attack. The correction has to happen at the level of the nervous system and the hormonal environment, not at the level of conscious muscular effort. This is why supported relaxation positions, where the body is held by gravity and external support rather than by muscular bracing, can do more for posture in 10 minutes than an hour of corrective exercises. When the nervous system feels safe and supported, it releases the flexion pattern on its own. You don't have to force extension. You have to create the conditions where the body chooses it.
This is why stress management is foundational for posture. The person who sleeps well, eats enough, breathes slowly through their nose, and has adequate thyroid function will always have better posture than the person grinding through corrections on five hours of sleep and discipline.
Part 7: Why Common Posture Corrections Cause Harm
With this framework in place, we can now look at the most common posture corrections and understand exactly why they fail. The problem isn’t that all corrective work is useless. Some targeted exercises can genuinely retrain the tonic system. The problem is how these cues are typically taught and executed: through voluntary bracing, forced positions, and recruitment of the wrong muscle layer. When a correction creates more tension and pain than relief, that’s a signal you’re overriding the system instead of supporting it.
“Pull your shoulders back.” This cue activates the rhomboids and middle trapezius to retract the scapulae. These are phasic muscles. They fatigue in minutes. Holding your shoulder blades pinned back creates constant tension across your upper back and can pinch the rotator cuff tendons where they pass under the bony tip of the shoulder blade. People who follow this advice chronically often develop burning between the shoulder blades, a sign of phasic muscle fatigue being mistaken for “weakness.”
Here’s what most people don’t know about scapular position: the shoulder blades naturally sit at about 30 degrees of protraction at rest. They’re supposed to lie gently against the posterior ribcage, slightly wrapped around the thorax, gliding freely over the serratus anterior. This is their healthy neutral position. When someone is told to “flatten” the blades against the back, they’re going past neutral into forced retraction, a position no muscle is designed to hold statically. The burning pain between the shoulder blades that so many people experience after “posture correction” is exactly this: phasic muscles in spasm from holding a position the body was never meant to maintain.
I know this pattern from the inside. In ballet, the aesthetic ideal demands maximally open, depressed, retracted shoulders. On stage, it’s stunning. In daily life, it’s a compressive, metabolically expensive brace that the body fights against the moment you stop consciously holding it. I spent years with that burning between my shoulder blades, thinking I needed to be stronger. I needed to let go.
The real issue behind rounded shoulders is usually an anteriorly tilted ribcage held up by accessory breathing muscles. The shoulders round forward because the ribcage is pulled up and forward by the scalenes and pectoralis minor, which are overworking because the diaphragm isn’t doing its job. Retracting the shoulders without addressing the ribcage position and the breathing pattern just creates a new layer of tension on top of the old one.
“Engage your core.” This typically means bracing the rectus abdominis and external obliques. Voluntary abdominal bracing increases intra-abdominal pressure artificially and compresses the spine. Done chronically, it creates a rigid, inflexible trunk that can’t adapt to changing loads. It also pushes downward on the pelvic floor, which is terrible for anyone with pelvic floor dysfunction, incontinence, or prolapse risk.
True core stability comes from the automatic, reflexive co-contraction of the transversus abdominis, multifidus, diaphragm, and pelvic floor. This is a pressure system, not a bracing system. It’s driven by proper breathing mechanics and proprioceptive input, not by conscious muscle squeezing.
“Stand up straight.” This cue has no anatomical specificity. People interpret it by extending their lumbar spine (increasing lordosis), lifting their chest (elevating the ribcage with accessory muscles), and locking their knees. The result is increased compressive load on the lumbar facet joints, compromised diaphragm position (because the ribcage is now in a fixed inspiratory position), and reduced blood flow to the lower extremities from locked knee positions. Soviet physical culture texts from the mid-twentieth century noted that even professional art models found the “correct upright stance” too fatiguing for sustained poses.
“Tuck your pelvis.” Posterior pelvic tilt flattens the lumbar lordosis, loads the posterior aspect of the intervertebral discs, lengthens the already-struggling lumbar multifidus, and inhibits the hip extensors (primarily the gluteus maximus). The lumbar curve exists for a reason: it distributes compressive loads across the disc surfaces and creates the space for the nerve roots to exit the spinal canal. Flattening it doesn’t “protect” the back. It destabilizes it.
Posture corrector devices. These external braces hold the shoulders in retraction passively. Over time, they cause the muscles that should be maintaining that position to atrophy further, because the mechanical demand has been removed. It’s the muscular equivalent of putting a healthy limb in a cast. When the brace comes off, posture is worse than before.
The litmus test. If a posture exercise creates tension, burning, or pain, you’re recruiting the wrong muscle layer. Corrective work that targets the tonic system should feel like relief, decompression, and opening. It should feel easier to hold yourself up afterward, not harder. If you feel worse after “correcting” your posture, the correction is the problem.
Part 8: What Actually Creates Good Posture
Good posture is an emergent property. You don’t build it. You create the conditions for it to happen. Those conditions operate across several layers, and each matters.