Several years ago, I fell while rock climbing and the sole of my foot landed against a sharp rock. The impact tore my plantar fascia. I had injuries before, torn ligaments and traumas accumulated over decades of ballet, training, and various athletic obsessions, but this one was among the most painful things I have ever lived through. It took months to get the right diagnosis. I kept being told it was something else. The recovery took close to a year, during which I could not lift, could not dance, could not move through any of the routines that had structured my life. I eventually healed. The small hardened nodule on the sole of my foot is still there, years later. It does not interfere with my life anymore, but on days when I pass roughly 20,000 steps, that foot starts to carry noticeably more tension than the healthy one. That injury sent me into the literature on what I had torn. What I found changed the way I understood my body and anatomy itself.
For most of the history of anatomy, students were trained to remove fascia and discard it. Scrape it off, cut it away, get to the “real” structures: the muscles, the bones, the organs underneath. The white tissue that wraps every muscle, surrounds every organ, sleeves every nerve, anchors every blood vessel, and connects all of it into one continuous fabric was treated as packing material. Robert Schleip, one of the leading fascia researchers in Europe, describes the conventional dissection process this way: classical anatomists were proud of removing this colorless sticky organ in order to handle the “actual” muscles and organs with care.
Fascia had a name long before modern anatomy learned to see it. It comes from Galen of Pergamon, the Greek physician who systematized Western anatomy in the second century AD.
Pseudo-Galen, Anatomia
He used it to name the attachments of muscles, and his texts on the structure and function of the body remained the standard medical reference for over a thousand years. Avicenna’s Canon of Medicine, written around 1025 in Persia, preserved and extended Galen’s anatomical framework and became the primary medical textbook in European universities for the next six centuries. When direct human dissection returned to Western anatomy through Vesalius at Padua in 1543, with the publication of De Humani Corporis Fabrica, the work that founded modern anatomy as a discipline, the lineage finally broke with the old texts. It also broke with what they had recognized about fascia.
Anatomical plates from Vesalius’ De Humani Corporis Fabrica
The new dissection-based anatomy treated connective tissue as obstruction to be scraped away. When the word entered English medical literature in the early 17th century, Helkiah Crooke, physician to King James I and author of Mikrokosmographia in 1615, described it as “the organ of the sense of touching.” Samuel Collins, physician to Charles II and later president of the Royal College of Physicians,devoted significant attention to the “membranes of the body” in his A Systeme of Anatomy of 1685 and described the connective tissue layers as “the garment of the body.”
Both descriptions were closer to what current research now shows than anything in standard twentieth-century anatomy textbooks. In 1800, the French anatomist Marie François Xavier Bichat, who founded histology as a discipline and reclassified the entire field of anatomy around tissue types, absorbed fascia into the broader category he called “cellular tissue.” His classification became the foundation of every modern anatomy textbook. Fascia lost its identity as a distinct system and was fragmented into named patches across the body. Microscopy turned the field’s attention to cells rather than networks. Formaldehyde embalming, which became standard in late 19th century dissection labs, dehydrated fascia and turned the living sliding tissue into the thick stiff layer that generations of medical students were taught to scrape away.
Medical specialization divided the body into organ systems that left no department responsible for the tissue connecting all of them. By the twentieth century, fascia was effectively invisible to mainstream medicine again. Now ask yourself which textbooks the doctor diagnosing your back pain studied from.
The rediscovery only began in 2007, with the first International Fascia Research Congress at Harvard, where Schleip, Langevin, Stecco, and other researchers met for the first time as a coherent field.
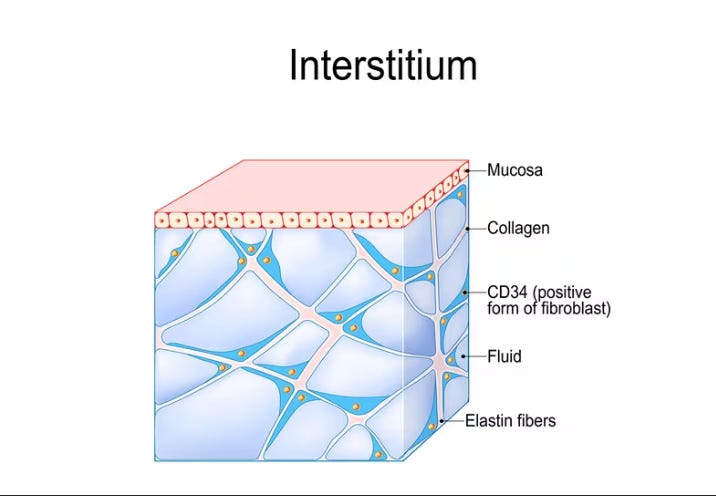
Eleven years later, that work hit the front page. In 2018, a pathology team at NYU School of Medicine published a paper in Scientific Reports arguing that the interstitium, the fluid-filled network of connective tissue threaded through every organ system, should be classified as the body’s 80th organ. The paper generated 2,400 news stories and roughly 3.8 billion online views. The same mistake the dissection labs had made with embalming, microscopy had been making for two centuries. When anatomists prepared tissue samples for microscope slides, they drained the fluid out of the sample. The fluid-filled compartments collapsed into what looked like dense connective tissue, and anatomy assumed that was the truth of the tissue. The whole field had been looking at corpses of fascia and calling it anatomy.
You have roughly the same volume of fascia as you have skeletal muscle. It contains more pain receptors than muscle does in some regions of the body. It contracts on its own in response to stress signals. Hormones rewrite its structure cycle by cycle. And nobody outside a small group of researchers thinks it matters very much.
Here is what depends on this tissue. How you move. How you breathe. How well your organs work. Posture. How fast you age and what your body looks like at fifty. How well your face holds its structure. The rate at which old injuries heal or refuse to heal. Whether your training builds you or breaks you down. Your mood, because fascia is wired to the sympathetic nervous system and chronic tension keeps that system switched on. Your digestion, because visceral fascia tension changes how your bile flows and how your intestines move. Your fertility and your menstrual cycle, because the pelvic organs sit inside a continuous fascial envelope. And yes, all the pain conditions too: chronic low back pain, frozen shoulder, plantar fasciitis, tennis elbow, sciatica with no clear disc cause, pelvic floor dysfunction, headaches that imaging cannot explain, fibromyalgia. The cascade of stiffness that arrives in your forties and never fully reverses.
This is the first piece in a series on fascia. It builds foundational knowledge. The pieces that follow go into hormones, hydration, pain, the visceral system, mechanical interventions, and the nutritional substrate that decides whether your connective tissue stays supple or hardens into the shape of every stress you have ever lived through.
In Padua, where Galileo lectured and Elena Cornaro Piscopia became the first woman in history to earn a university doctorate, a family of anatomists has been quietly correcting Vesalius’s legacy for two decades. Carla Stecco, professor of anatomy at the University of Padua, published the first comprehensive Functional Atlas of the Human Fascial System in 2015. Her brother Antonio Stecco works on the clinical side at New York University. Their father Luigi was the originator of the family’s fascial work. Carla’s atlas is now the reference text for anyone doing serious fascial research.
What she and others have shown is that fascia is not one tissue. It is a continuous, layered system that wraps and connects everything. There are at least five fascial systems in the body, and they are all physically continuous with each other.
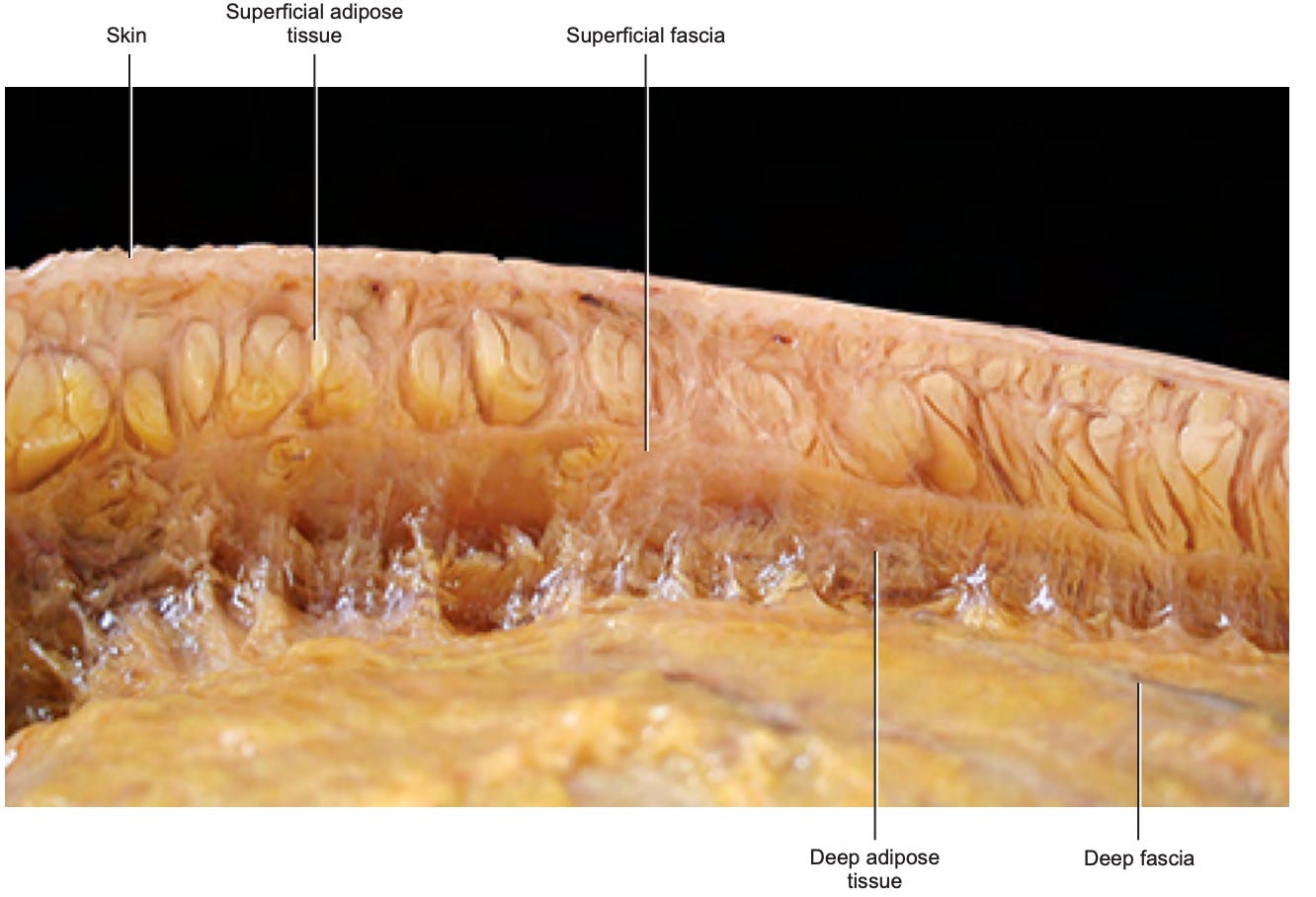
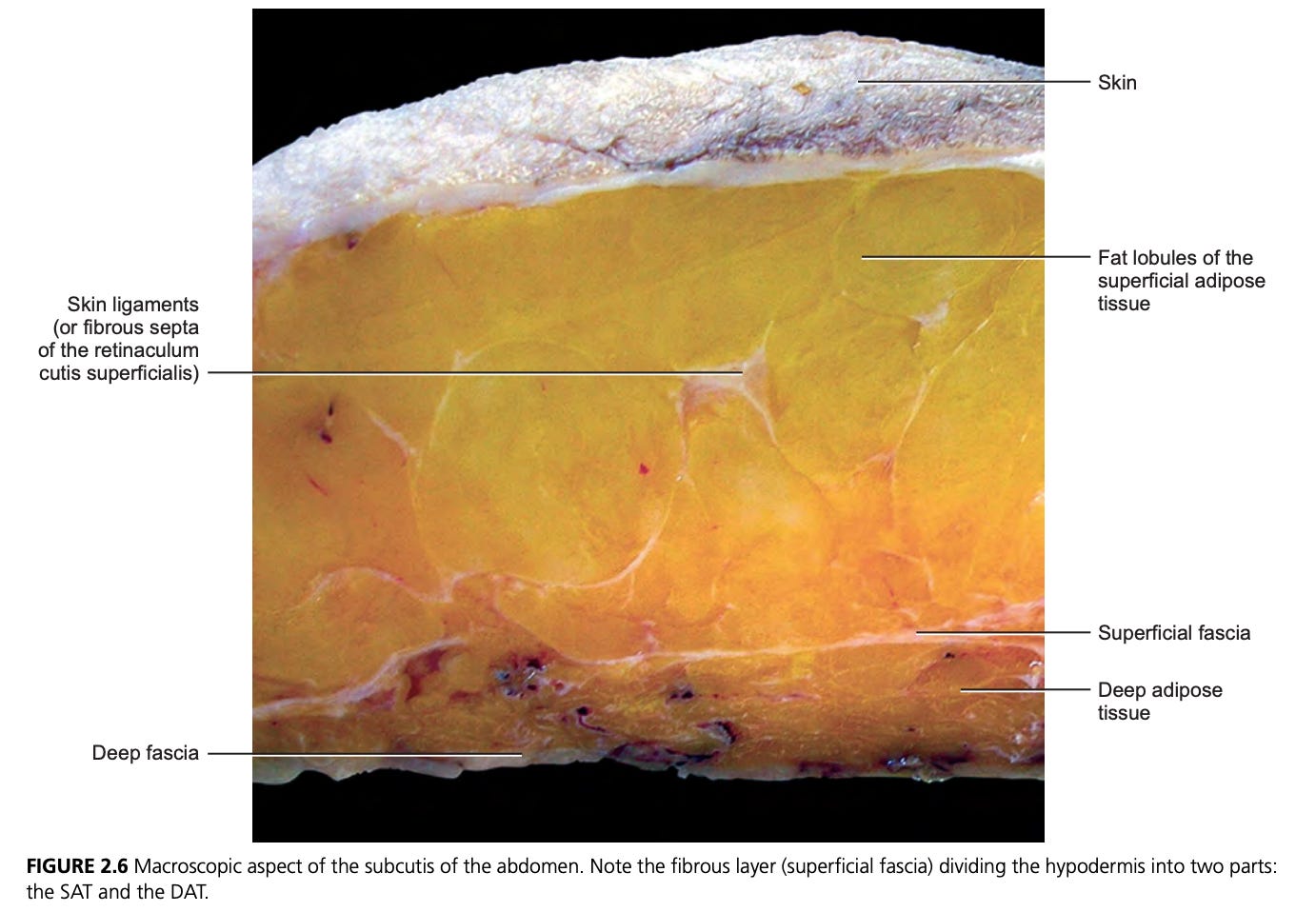
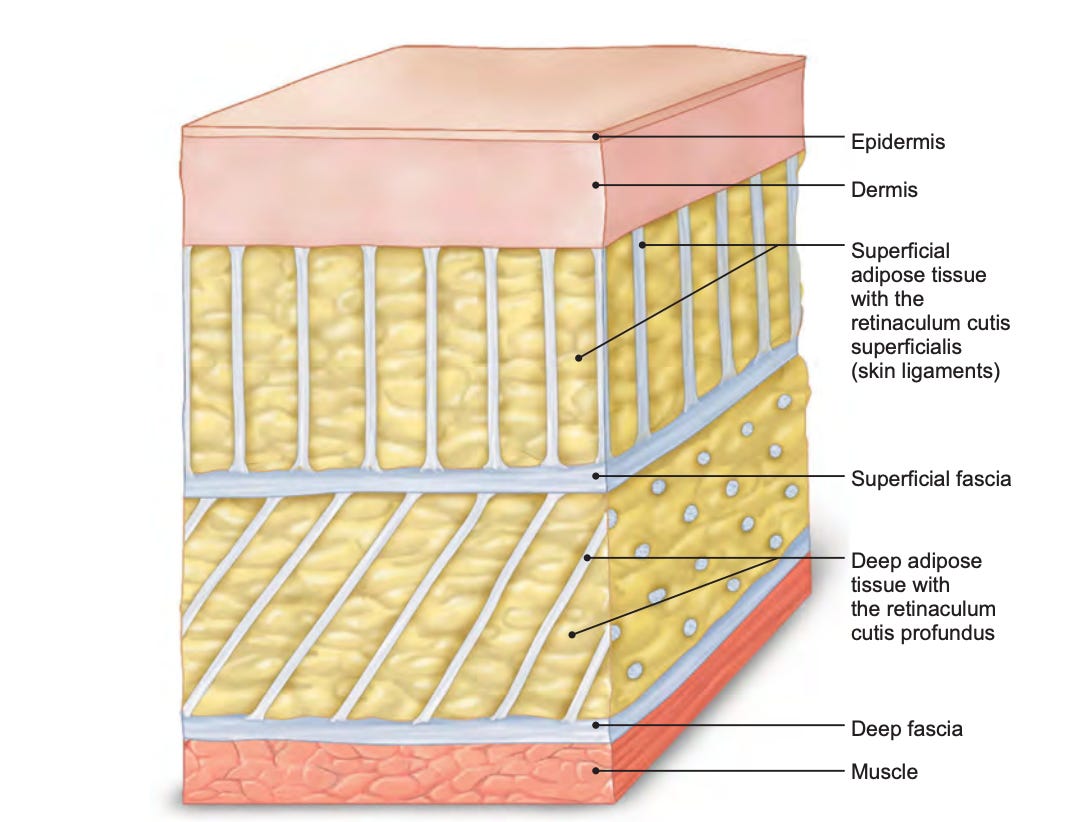
Superficial fascia sits just under the skin. It contains adipose tissue, lymphatic vessels, and a dense network of nerve endings. Stecco’s group documented nerve structure density in the superficial fascia at 33 to 64 per square centimeter. That makes it the second most highly innervated soft tissue in the body after the skin itself.
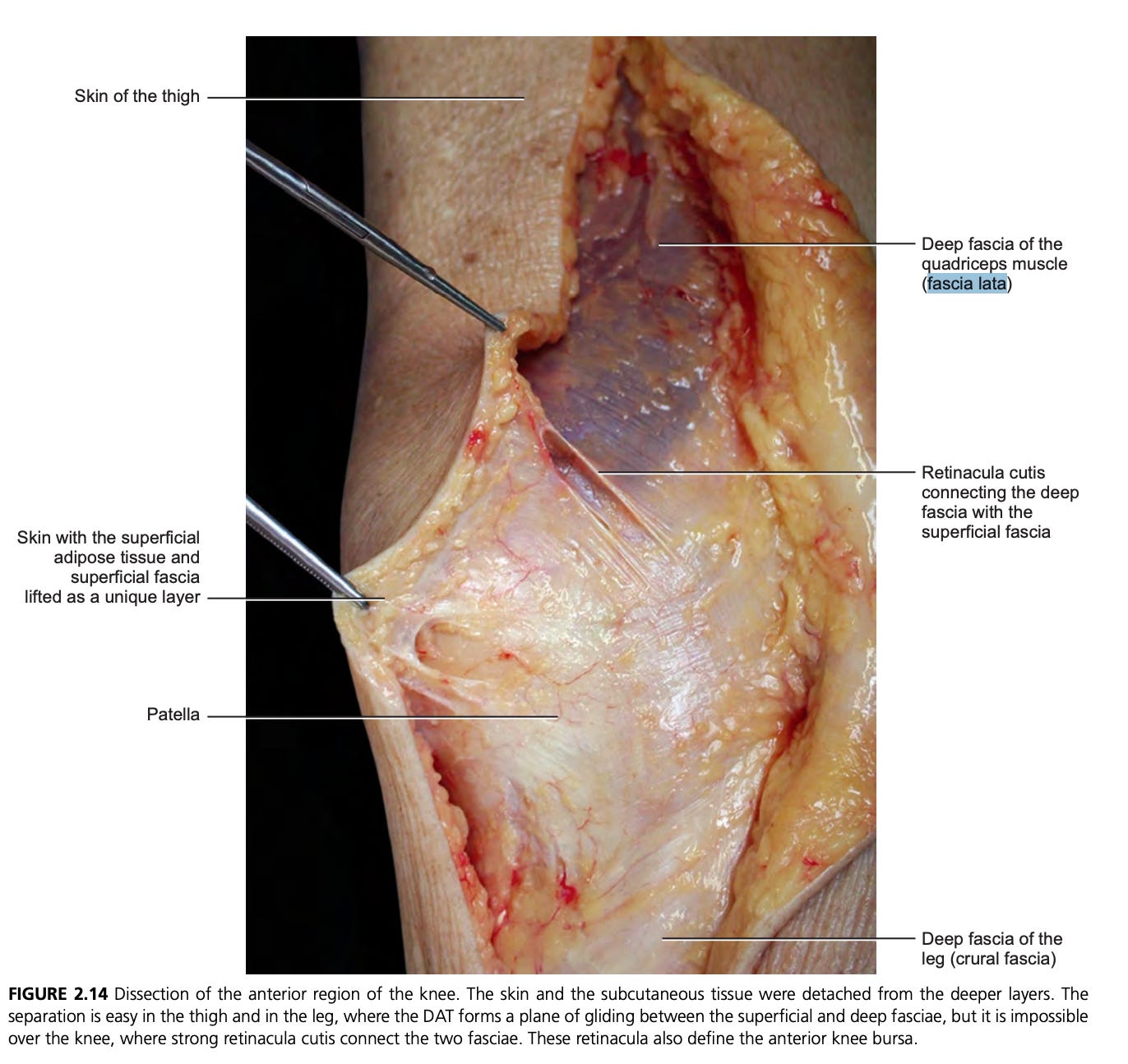
Deep fascia is the dense, fibrous, white tissue that wraps every muscle and bundles muscles into functional groups. It also extends inward to separate muscles from each other, creating sliding planes that allow tissues to move independently. The fascia lata of the thigh and the thoracolumbar fascia of the lower back are deep fascias. They look more like cellophane than rope. Under a microscope, they reveal layered collagen sheets oriented in different directions, with thin layers of loose connective tissue and hyaluronic acid (HA) between them that allow sliding.
Stecco C. Functional Atlas of the Human Fascial System. Elsevier, 2015. Used for educational commentary.
Visceral fascia wraps your organs. Liver, kidneys, intestines, bladder, uterus, lungs, heart. Each organ has its own fascial envelope, and these envelopes connect to each other through ligaments and mesenteries. Tension in one part of the visceral fascial system pulls on neighboring organs. This is the territory of Jean-Pierre Barral’s visceral manipulation lineage and, in a different tradition, of Alexander Ogulov’s Slavic abdominal work. My earlier piece on visceral self-massage walks through both lineages and the practical techniques.
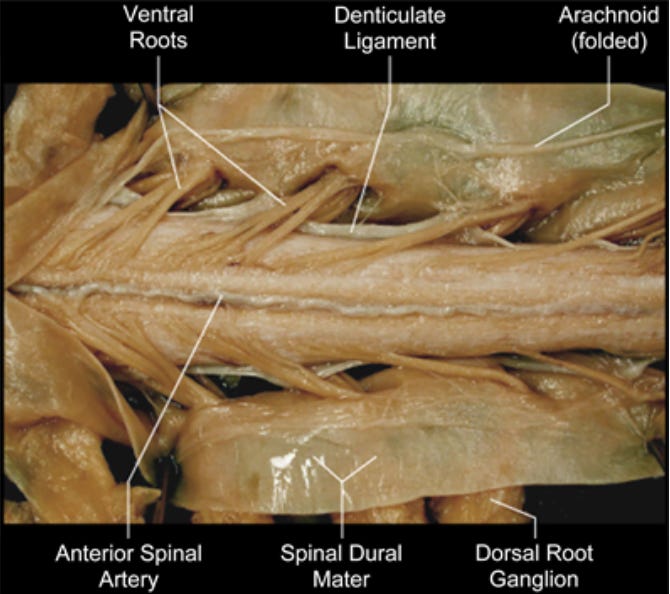
Neural fascia surrounds every nerve in the body. The endoneurium, perineurium, and epineurium are connective tissue sleeves at progressively larger scales. When fascia densifies around a nerve, the nerve gets compressed, and you get the symptoms anyone with sciatica or carpal tunnel will recognize: tingling, numbness, weakness, electric pain.
Dural fasciawraps your brain and spinal cord. It runs from the base of your skull, down the entire spine, and anchors at the tailbone, where it becomes continuous with the fascia of your pelvic floor. The membrane around your brain and the floor of your pelvis are one connected tissue. The full implications of this, including the way small muscles at the base of the skull pull directly on the membrane around your brain to generate certain kinds of headaches, are too rich for this section. The pain piece later in this series will go deeper.
The crucial point is that these systems are not separate sleeves stacked on top of each other. They are physically continuous. The body, viewed through the fascia, is a single connective tissue continuum from skull to sole.
Guimberteau’s footage and the living network
Anatomy textbooks always show fascia as flat, two-dimensional drawings. The reality is something else entirely. In Bordeaux, Jean-Claude Guimberteau, a hand and reconstructive surgeon, developed a technique for filming living fascia during surgery. He inserted small endoscopic cameras into open surgical fields and recorded what fascia looks like when it is alive, hydrated, and moving.
His footage changed how serious researchers think about this tissue. Fascia is not flat sheets. It is a chaotic-looking, fractal, fibrillar network of fibers running in every direction, surrounding fluid-filled microvacuoles. There are no empty spaces. Everything is connected to everything through this dense, irregular mesh. When the tissue moves, the fibers slide past each other, reorganize, and settle into new arrangements without losing their connections.
If you watch his footage with the eyes of someone who has been told the inside of the body is mostly empty space, you have to update your model. There is no empty space. The fascial continuum fills every gap, surrounds every structure, and provides the mechanical and biochemical medium in which everything else floats. The cells and organs of the body do not sit in space. They sit in fascia.
This matters for how you interpret pain, dysfunction, and recovery. If fascia is continuous, then a problem in one location can pull on, irritate, or compromise something far away. Your body does not have isolated parts. It has one connective tissue system, and that system communicates mechanically and chemically with itself across the whole organism.
Force travels through your body
The anatomy of fascia is no longer obscure. The Stecco atlas covers it in detail. What is still being mapped is how fascia organizes into specific long-distance chains through which force travels across the whole body.
In Frankfurt, a research group led by Jan Wilke at the Goethe University took the question of fascial continuity into the lab. Thomas Myers, an American bodyworker, had proposed in his book Anatomy Trains that the body’s fascia organizes into “lines” or “chains” through which mechanical force can travel. Pull on one part of the chain, the rest responds. Myers himself was open about the fact that his model was hypothesis, not established anatomy. Wilke set out to test it.
Thomas Myers Anatomy trains
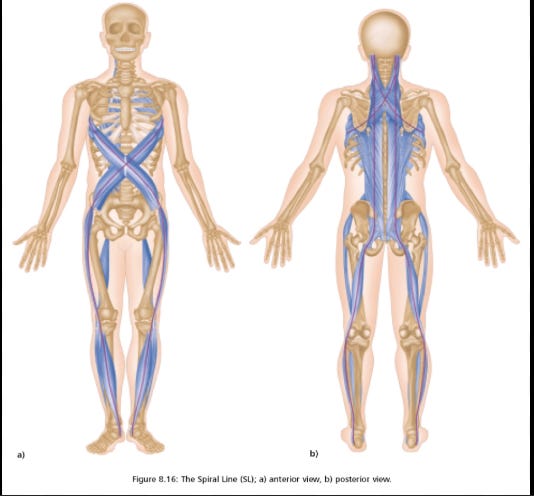
His 2016 systematic review in Archives of Physical Medicine and Rehabilitation looked at six proposed myofascial chains and analyzed 62 cadaver dissection studies. Three chains showed strong end-to-end evidence: the superficial back line (the most well-documented, with 14 supporting studies), the back functional line, and the front functional line. Two chains showed partial evidence: the spiral line, with 5 of 9 transitions verified across 21 studies, and the lateral line, with 2 of 5 transitions verified across 10 studies. These are not speculative. They are partially confirmed, with some segments anatomically verified and others still requiring evidence.
The broader myofascial-chain model is still being debated and refined. Some chains have anatomical support. Some have partial support. One did not hold up well. The superficial front line, which Myers proposed connects the rectus abdominis to the rectus femoris, showed no clear fascial continuity across the abdomen in the studies Wilke reviewed. That does not mean the front of the body is not functionally connected. It means this specific direct fascial bridge was not anatomically confirmed. The regions may still interact through adjacent fascial layers, muscles, tendons, pressure systems, motor control, and movement patterns.
Later work has continued to sort the model line by line rather than accepting or rejecting it as a whole. A 2025 follow-up review confirmed several previously described fascial continuities and added new evidence for a neck-eye fascial continuum, with connections traced from the muscles at the back of the skull through the scalp aponeurosis to the muscles around the eyes. This is one mechanistic reason why neck tension and eye strain often travel together.
The functional implications are where this gets interesting. In a 2017 randomized controlled trial published in the Journal of Sports Sciences, Wilke and his team tested whether stretching the lower limb would improve cervical (neck) range of motion. They divided 63 participants into three groups: one group stretched the hamstrings and calves, one group stretched the neck directly, and a control group did nothing. Both stretching groups improved cervical range of motion compared to the control. The two stretching protocols produced similar results.
Read that again. Stretching the hamstrings produced the same improvement in neck mobility as stretching the neck. The mechanical effect traveled the length of the body through the superficial back line. Earlier work by the same group recorded a 6.22 degree improvement in cervical sagittal range of motion after hamstring stretching alone.
When you treat your body as a collection of independent muscles and joints, this finding makes no sense. When you treat it as a continuous fascial system, it is exactly what you would predict.
It also rewrites what we should be thinking about with persistent pain. Many people with plantar fasciitis improve faster when their therapist works on the calf, hamstring, and lower back, not the foot. People with neck pain sometimes respond to lower-limb mobility work better than to direct neck treatment. Tom Myers describes how rarely he gets durable improvement in plantar fasciitis by treating the foot alone, and how often working the back of the leg or the occiput produces lasting change. The body is not separate parts.
Fascia tensions itself
Now we get to the finding that broke my mental model when I first encountered it. Fascia contracts. Independently of muscles and nerves.
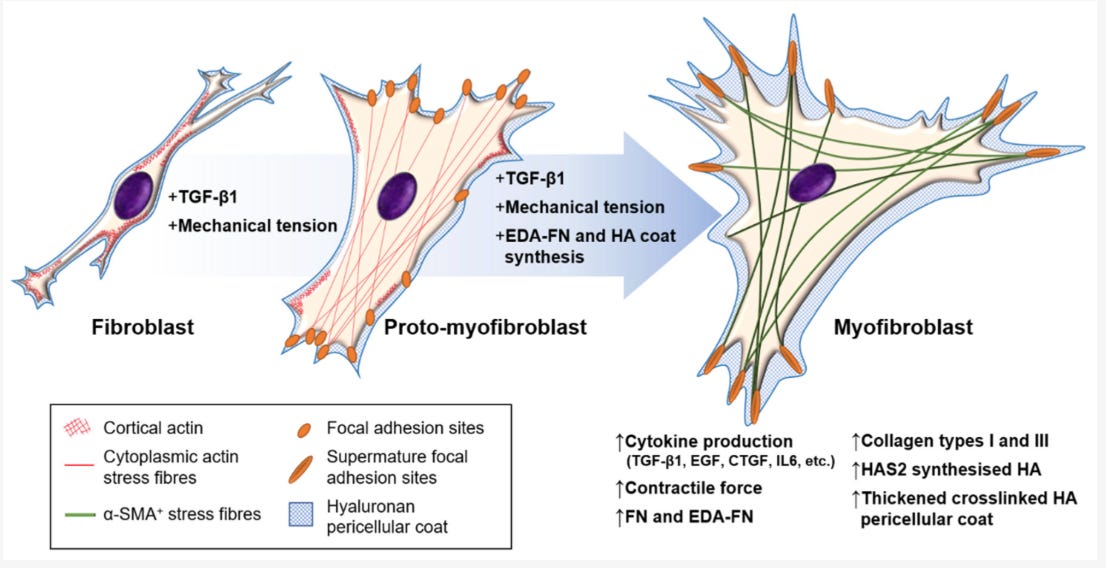
Robert Schleip and his collaborators at Ulm University published a hypothesis paper in 2005 arguing that fascia might contain enough contractile cells to actively generate tension, independent of the muscle fibers it wraps. By 2019, with a paper in Clinical Anatomy titled “Active contractile properties of fascia,” they had the mechanographic evidence. They cut strips of human thoracolumbar fascia, placed them in an organ bath, and tested how they responded to various chemical signals. The fascia contracted in response to transforming growth factor beta-1 (TGF-β1), a fibrogenic signaling molecule released during chronic stress and inflammation. It also contracted in response to fetal bovine serum and certain other agents. It relaxed in response to a Rho-kinase inhibitor.
The cells driving this contraction are myofibroblasts. They are fibroblasts that have differentiated into a more contractile state by expressing alpha smooth muscle actin (α-SMA). Schleip’s group documented their density in the human thoracolumbar fascia at an average of 79 cells per square millimeter. They contract slowly and hold tension for long periods, behaving more like smooth muscle than like skeletal muscle. They are the cells responsible for wound contraction during healing. They are also the cells responsible for pathological fascial contractures.
The same cell type drives Dupuytren’s contracture in the palm of the hand, plantar fibromatosis (Ledderhose disease) in the foot, frozen shoulder in the joint capsule, and a range of other conditions where fascia progressively tightens, thickens, and refuses to release.
Dupuytren’s contracture
The hardened nodule on the sole of my foot is downstream of the same biology, except my trigger was not spontaneous fibromatosis. It was trauma, followed by bad medicine. The mass formed at the exact site where my plantar fascia tore, and it is the direct result of three months of walking on a torn fascia while being told nothing was wrong. The X-rays came back clean. I was told to keep walking on it. X-rays show bone. They cannot show fascia. A plain film of a torn plantar fascia looks identical to a plain film of a healthy one, which is why MRI or ultrasound is the standard imaging for this diagnosis. It took three months of escalating pain before they finally ordered the MRI that confirmed the rupture. The actual treatment for an acute plantar fascia tear is non-weight-bearing immobilization for six to twelve weeks while the tissue knits cleanly. Walking on torn fascia during that window forces the body to repair under continuous mechanical insult. The torn ends never get close enough to heal together. Fibroblasts deposit collagen in random orientations. Myofibroblasts activate aggressively and contract the wound permanently. By the time the correct diagnosis arrived, the tissue had laid down a mass of disorganized fibrotic collagen at the rupture site that no amount of subsequent rehab was going to fully reverse. My nodule exists because the doctors who saw me were incompetent at diagnosing soft tissue injury.
The same TGF-β1 signal that triggered the lab fascia to contract in Schleip’s experiments gets released throughout your body in response to chronic inflammation, tissue irritation, and the cumulative effects of sustained stress. Chronic stress is one of the major drivers, working through a cascade that involves chronic low-grade inflammation, sympathetic activation, oxidative stress, and the glucocorticoid resistance that develops when cortisol stays elevated too long. Blood sugar dysregulation and chronic infection push the system in the same direction. Hypothyroidism slows the resolution of these signals. Chronically high estrogen, without enough progesterone to balance it, makes connective tissue dense and stiff. Your body is responding to its metabolic and hormonal environment by tightening its connective tissue, cell by cell, year by year.
This is the mechanism for what people describe as “I just feel tight everywhere all the time.” Myofibroblast activation drives it. The fascia is doing exactly what a tissue with internal smooth-muscle-like contractile machinery would do under chronic inflammatory and hormonal stress. It tightens. It holds. It refuses to let go.
And the contraction is not under voluntary control. You cannot relax your fascia by deciding to relax. The signal that drives the contraction is biochemical, which means the trigger does not come through the motor nerves that you can consciously command. You can lie completely still on a beach in Italy and your fascia will still tighten if TGF-β1 is being released somewhere in the body.
The most sensitive tissue you have
Through the 2010s, a research team led by Siegfried Mense in Mannheim, Germany, set out to determine whether fascia is actually a source of pain or just a passive structure that pain travels through. The question matters. If fascia is densely innervated with nociceptive (pain-sensing) nerves, then much of what people call “muscle pain” might actually be fascia pain. If it is not innervated, then the conventional muscle-and-joint model of back pain stays intact.
The team performed quantitative histology on the thoracolumbar fascia in rats and on samples of the human thoracolumbar fascia. Their 2011 paper in Neuroscience, lead-authored by Jonas Tesarz at Heidelberg, documented dense networks of substance P-positive and calcitonin gene-related peptide (CGRP) positive free nerve endings throughout the fascia. Substance P is the classic neuropeptide associated with nociception (the detection of tissue damage) and inflammation. Its presence indicates that the fascia is actively wired to detect tissue damage and inflammatory signals.
The density varied by layer. The outer (superficial) layer of the thoracolumbar fascia and the subcutaneous tissue immediately above it showed the highest concentration of nociceptive fibers. The middle layer had fewer. The inner layer, adjacent to the multifidus muscle, had moderate density.
In follow-up work, Mense’s group induced experimental inflammation in the fascia and showed that the density of CGRP and substance P positive nerve fibers increased after inflammation. That is the structural signature of sensitization. The tissue becomes more pain-sensitive, more responsive to small mechanical stimuli, and more prone to send pain signals to the central nervous system.
A study by Schilder and colleagues in 2014 tested this directly in human volunteers. They injected hypertonic saline into either the muscle, the muscle fascia, or the subcutaneous tissue and asked subjects to rate the pain. Fascia injection produced higher pain ratings than muscle injection. The thoracolumbar fascia had a lower pain threshold than the underlying muscle. When you press into your back and it hurts, the pain is more likely coming from the fascia than from the muscle.
This rewrites a lot of clinical thinking about chronic back pain. Most patients with persistent low back pain have unremarkable imaging. The disc looks fine. The vertebrae look fine. The nerves look fine. The current best evidence is that a large fraction of this “nonspecific” low back pain is actually fascial pain. The structural model of pain (something is bent, displaced, or damaged) does not apply, because fascia generates pain through a different mechanism: densification, restricted sliding, inflammatory sensitization of nociceptors, and the activation of sympathetic nerve fibers embedded in the fascial layers.
Schleip and others have shown that the fascia is also densely innervated with sympathetic nerve fibers. These are the fibers of the autonomic nervous system that respond to stress. When you experience chronic stress, sympathetic activity rises. Sympathetic fibers in the fascia release norepinephrine and related signaling molecules, which alter blood flow, tissue tone, and inflammatory state in the local fascial environment. This is the mechanistic bridge between emotional stress and chronic physical tension that most people feel but cannot explain.
You have lived this. The week you cannot sleep because of family stress, your back tightens. The job that runs you down for years gives you the chronic neck and shoulder pattern you cannot stretch out. The tension is not in your imagination. It is in your fascia, driven by sympathetic activation, sensitized nociceptors, and myofibroblast-mediated contraction.
Fascia is a water organ
Live fascia is mostly water. Depending on age, hydration status, and metabolic context, fascia is approximately 60 to 70 percent water by composition. That water is held in a structured form by hyaluronic acid (HA), a polysaccharide molecule with a remarkable property: it binds up to ten times its dry weight in water and forms a viscous, slippery gel.
Hyaluronic acid is the lubricant of the fascial sliding planes. Between every fascial layer, between deep fascia and the muscle it wraps, between adjacent muscles that need to slide past each other during movement, there is a thin film of HA-rich loose connective tissue. When the HA is well hydrated and at the right molecular weight, the fascia slides. Movement is fluid, range of motion is full, and the body feels light. When the HA aggregates into longer chains, becomes more viscous, or loses water, the fascia stops sliding. This is what Stecco’s group calls densification, and it is one of the dominant mechanisms of stiffness and chronic musculoskeletal pain.
The cells that produce this HA were identified by the Stecco group in 2018 in a paper in Clinical Anatomy. They named them fasciacytes, a distinct cell type related to but different from ordinary fibroblasts. Fasciacytes are plumper, more secretory, and immunologically distinguishable. They live in the loose connective tissue layers between fascial sheets, and their primary job is to maintain the HA-rich gel matrix that enables sliding.
What disrupts HA quality and quantity? Several things. Prolonged immobilization is one. When you hold the same posture for hours, the local HA aggregates and increases in viscosity, and the tissue stops sliding well. This is the mechanism behind the morning stiffness you feel after sleeping in one position, and behind the back tightness you develop after eight hours at a desk. It is also the mechanism behind a longer-term consequence: a body that does not move through full ranges of motion regularly will progressively densify its fascia over months and years.
HA viscosity decreases at higher temperatures. This is part of why warm baths, saunas, and warm-up movement loosen the body. The fascia literally becomes more fluid at higher temperatures.
Pressure and shear matter. Fasciacytes respond mechanically. When you apply slow, sustained pressure or shearing motion to a region of densified fascia, the fasciacytes are stimulated to produce fresh HA, and the older aggregated HA is broken up. There is a specific deep friction technique designed to exploit this.
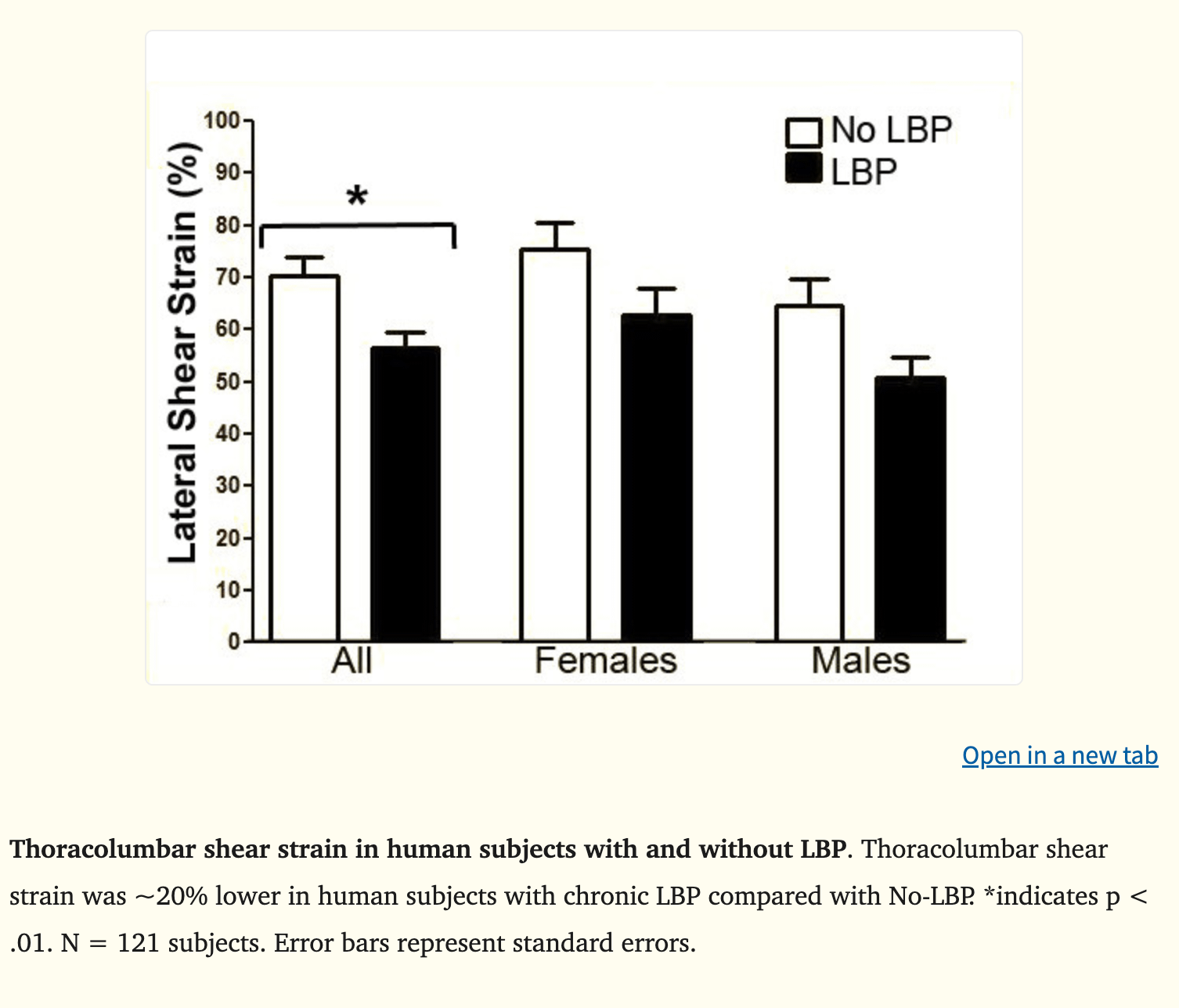
Helene Langevin at Harvard published a key piece of this in 2011 in BMC Musculoskeletal Disorders. Her team used ultrasound elastography to measure fascial shear strain in 121 subjects: 50 without low back pain, 71 with chronic low back pain. The fascia of the chronic pain group had approximately 20 percent lower shear strain than the controls. Their fascia slid less. The tissue was denser, more restricted, less fluid. This finding has been replicated, refined, and extended by other groups in the years since.
The same researcher’s earlier work documented what happens when fascia is immobilized in rats. After three weeks of restricted movement, the tissue thickens, the collagen pattern becomes disorganized, and the structure begins to resemble pathological fibrosis. After active stretching, both passive and externally applied, the fibroblasts in the tissue elongate dramatically, release relaxing signals, and the tissue softens. The change is structural and measurable.
Your tissue is alive. It responds to what you do with it. If you do not move it, it locks down. If you move it across full ranges with appropriate load, it stays fluid. Movement is only part of the picture.
The fluid quality of your fascia also depends on signals that arrive from inside the body, written by hormones that change cycle by cycle and decade by decade.
The hormonal organ
Until about 2016, almost no one was looking at fascia from a hormonal standpoint. Then Caterina Fede in Carla Stecco’s lab in Padua started running immunohistochemistry on human fascial tissue samples and asking whether the cells expressed receptors for the major sex hormones. Her 2016 paper in the European Journal of Histochemistry was the first to demonstrate that human fascial fibroblasts express estrogen receptor alpha (ERα) and relaxin receptor 1 (RXFP1). The fascia is a hormonally responsive tissue.
She extended this work in 2019 with a paper in PLoS One. The team took fascial cells from human samples and put them in a dish with the levels of estrogen and relaxin that match different phases of a woman’s cycle: follicular, ovulation, luteal, postmenopausal, and pregnancy. The cells changed how much structural protein they produced based on which hormones were in the dish. When the estrogen level matched ovulation, the cells made roughly two thirds less collagen-I than they did at follicular phase levels. Estrogen tells fascial cells to slow down on collagen. Relaxin, the hormone that rises sharply in pregnancy, pushes them even further in the same direction. Both hormones reshape the building blocks of connective tissue cycle by cycle, and across the lifespan.
Women experience musculoskeletal pain at higher rates than men. Women have higher rates of fibromyalgia, chronic neck pain, low back pain during pregnancy, frozen shoulder during the perimenopausal transition, and pelvic floor dysfunction across the lifespan. The fact that fascia is one of the major tissues mediating these conditions, and that fascia responds directly to estrogen and relaxin levels, is not a coincidence.
The perimenopausal window is particularly informative. As estrogen levels drop and become erratic, collagen turnover in the fascia and tendons becomes disorganized. The fascial system becomes less compliant in some women and more lax in others, depending on the dominant hormonal trajectory. Frozen shoulder rates spike in women in their late forties and early fifties, almost certainly because of these fascial changes. Pelvic floor fascia changes underlie much of the postmenopausal pelvic pain and prolapse pattern.
The same Stecco group also identified cannabinoid receptors (CB1 and CB2) on fascial fibroblasts. Fascia is responsive to endocannabinoid signaling. The relevance of this for chronic pain, for the analgesic effects of certain massage and bodywork techniques, and for the broader anti-inflammatory tone of the body remains an active area of research that the pain piece later in this series will cover in depth.
Thyroid hormone runs the fluid quality of the fascia from a different direction. Triiodothyronine (T3) normally inhibits the activity of hyaluronan synthetase and accelerates the degradation of older HA molecules, which keeps the gel between fascial layers at the right viscosity. In hypothyroidism, the system runs the opposite way. HA accumulates in a denser, less mobile form. The accumulation is the underlying mechanism of myxedema, the classic skin and connective tissue change of low thyroid. The tissue looks thick. The face puffs. The lower legs swell in a way that does not pit on pressure, because the extra fluid is bound to HA rather than free. Full clinical myxedema is rare. Suboptimal T3 is common, and the fascial consequence is exactly what the mechanism predicts: progressive HA accumulation in the wrong form, declining tissue fluidity, slow loss of the gliding properties of the fascial system, and stiffness that does not respond to stretching because the problem sits at the level of tissue hydration and HA quality.
T3 also suppresses SMAD activation in the TGF-β1 pathway, which limits the transition of fibroblasts into myofibroblasts. And T3 is required for normal collagen turnover. Without adequate T3, old, glycated, poorly organized collagen accumulates and the tissue becomes brittle, dense, and prone to chronic inflammation.
Hypothyroid bodies are stiff bodies. The fascia cannot stay fluid.
Cortisol is the destructive counterpart. Chronic cortisol elevation drives the TGF-β1 pathway, increases myofibroblast activation, breaks down structural collagen while encouraging its disorganized rebuilding, and shifts the tissue toward exactly the pathology that defines chronic musculoskeletal pain syndromes. If you have lived through a sustained period of high stress and noticed that you came out of it physically tighter, more pained, and less mobile, you are observing this process directly.
Insulin and blood sugar matter too. Hyperinsulinemia drives glycation of collagen, producing advanced glycation end products (AGEs). AGE-modified collagen is stiffer, more brittle, less repairable, and more resistant to normal turnover.
Polyunsaturated fatty acid (PUFA) accumulation in connective tissue is the other slow-burning damage process. PUFAs in tissue oxidize over time, generate lipid peroxidation products, and slowly turn the collagen environment more damaged. The connective tissue ages faster, becomes less responsive, and contributes to the diffuse stiffness that everyone over forty notices but few can explain.
Fascial quality is metabolic quality. Fascia is a hormonally regulated, metabolically sensitive, fluid-dependent organ system. Its quality at any given moment reflects your thyroid status, your sex hormone balance, your cortisol load, your blood sugar regulation, and your dietary fatty acid profile. The vague aches and stiffness most adults carry are the cumulative readout of decades of fascial response to the metabolic environment. Calling it “getting older” obscures the mechanism. The substrates and signals that determine cellular metabolism are the same substrates and signals that determine fascial quality. You cannot fix the fascia downstream while ignoring the upstream chemistry.
One body, one tissue
The visceral fascia is the section of the system that connects everything to digestion, hormones, and pelvic stability. Your diaphragm is a sheet of muscle and tendon, but it sits inside continuous fascial attachments. The central tendon of the diaphragm is connected through the pericardium (the fascial sac around the heart) upward to the cervical fascia at the base of the neck. Through its crura and posterior attachments, it is connected to the lumbar spine, the psoas, the quadratus lumborum, and the retroperitoneal fascia that wraps the kidneys, the great vessels, and the lumbar nerve plexuses.
Below the diaphragm, the fascial system continues. The omentum and mesenteries suspend and connect the digestive organs. The renal fascia wraps the kidneys and adrenals. The pelvic fascia anchors the bladder, the uterus and ovaries, the prostate, the rectum, and the pelvic floor musculature. The endopelvic fascia connects laterally to the obturator internus and inferiorly to the levator ani and coccygeus. Every organ in your abdomen and pelvis sits inside a fascial envelope that connects to every other envelope.
This continuity is why a tight pelvic floor changes the way you breathe, and why restricted diaphragm motion is so often associated with sluggish digestion, poor bile flow, and pelvic pain. The whole front of the trunk is one fascial system. When one region restricts, the others have to compensate.
The dura extends the continuity further still. Beyond the skull-to-pelvis anatomy, the dural system also holds the cranial bones to each other through internal attachments and links the cranium to the sacrum as a single mechanical unit. Tension at one end is, at minimum, transmissible to the other.
This is why fascia matters. It is the medium through which everything in the body relates to everything else. Mainstream medicine learned to study tissues by isolating them. Fascia cannot be understood that way, because its function is connection itself. The reductionist anatomy of the last four centuries gave us extraordinary knowledge of bones, muscles, organs, and biochemical pathways. It also gave us a body that doesn’t quite hang together, because the tissue that holds it all together was the one we threw away.
What this series will do
The pieces that follow will build out the fascia story one mechanism at a time.
What changes fascia. What damages it. What keeps it fluid. What makes it harden.
The science is still catching up to the obvious fact that the tissue anatomy discarded was shaping far more than anatomy. The clinical implications are still emerging. But the old model is already dead. Fascia is not packing material or some passive wrapping. It is a sensory, contractile, hormone-responsive, stress-responsive, metabolically sensitive organ system.
This series is my attempt to put it back where it belongs: at the center of how we think about pain, posture, aging, movement, stress, and the body’s ability to hold itself together, or slowly lose that ability, over time.
I’m honestly in awe of all this information and overwhelmed in the best way. You put so much work into this. I’m going to print it and read it carefully over the weekend 🙏🏻❤️
I discovered many year ago, through a treatment for an old injury, that it was the fascia causing the grief in my knee and not the meniscus. It was a treatment from a woman who practices and teaches Ortho-biology.
My current Osteopath also treats at the fascia level.
And my chiropractor has training on the importance of fascia.
It's extraordinary.
And I have talked with another practitioner who believes it's fascia, when twisted and injury untreated, that can cause people to hunch over later in life.






I’m honestly in awe of all this information and overwhelmed in the best way. You put so much work into this. I’m going to print it and read it carefully over the weekend 🙏🏻❤️
I discovered many year ago, through a treatment for an old injury, that it was the fascia causing the grief in my knee and not the meniscus. It was a treatment from a woman who practices and teaches Ortho-biology.
My current Osteopath also treats at the fascia level.
And my chiropractor has training on the importance of fascia.
It's extraordinary.
And I have talked with another practitioner who believes it's fascia, when twisted and injury untreated, that can cause people to hunch over later in life.